From Clinic to Community: Making Care Work
Imagine trying to manage diabetes while living out of your car. Or showing up to a doctor’s appointment after skipping meals for days. These aren’t rare scenarios they’re everyday realities for millions of Americans. And yet, most care plans barely acknowledge them. That disconnect is exactly what the Accountable Health Communities model set out to fix.
It wasn’t about adding more tests or prescriptions. It was about asking the right questions like “Do you have food in the fridge?” or “Can you get to your appointments?” It challenged the system to see patients as people, not just problems to solve.
But shifting from intention to impact is harder than it sounds. Now, as ACOs take the baton, the challenge is clear: how do we truly integrate social care into healthcare—and do it at scale? To understand why this model matters and why it struggled let’s break down how the Accountable Health Communities (AHC) model was designed to work. This post dives into what we’ve learned and what comes next in making that vision a reality.
What Is the Accountable Health Communities Model?
At its core, the Accountable Health Communities model (AHC) is all about connecting the dots between a person’s clinical care and the real-life challenges they face outside the exam room things like not having a ride to the doctor, running low on food, or living in an unstable home. It’s a bold idea launched by the CMS Innovation Center in 2017 with a clear goal: to test if identifying and addressing these health-related social needs (HRSNs) could actually improve health outcomes and lower costs (Johnson et al., 2022).
The model focused on three main strategies:
- Screening Medicare and Medicaid patients for key social needs
- Referring them to local community services
- Navigating those patients through the system to get their needs met
Sounds simple, right? In practice, it’s anything but. As the studies and CMS evaluations show, connecting healthcare with social care isn’t just about handing someone a brochure. It requires infrastructure, coordination, and trust three things often in short supply across fragmented U.S. healthcare systems.
Where Did the AHC Model Struggle?
The vision was compelling, but execution brought a new set of headaches. Several roadblocks kept this model from fully delivering on its promise. Let’s look at the major issues that emerged across the five-year pilot.
1. Navigation Alone Isn’t Enough
Even when patients were assigned navigators, it didn’t guarantee their social needs would be resolved. In fact, according to a 2023 Health Affairs study, patients who received navigation support weren’t any more likely to connect with community resources than those who didn’t. Why? Many communities simply didn’t have enough services to go around (Parish et al., 2023).
Imagine being handed a map to buried treasure only to find the treasure chest is empty. That’s what it felt like for many patients trying to get help with housing, transportation or mental health services. Navigation without available resources becomes a frustrating loop.
2. Disconnected Data Systems
Another common challenge in the Accountable Health Communities model was the lack of integration between healthcare and social service data systems. Clinicians often never saw screening results because they weren’t included in the electronic health record (EHR). That meant care teams were flying blind when it came to their patients’ biggest barriers to care (Johnson et al., 2022).
Think about it: would you send a pilot up in the air without radar? That’s what it’s like trying to deliver whole-person care without access to SDOH data.
3. Poor Feedback Loops
Tracking whether patients actually received services or whether those services helped was a huge challenge. Without closed-loop referral systems in place, there was no easy way to confirm if needs were met. This made it tough to hold providers or community organizations accountable, much less improve performance over time (Renaud et al., 2023).
Why ACOs Are Perfect for Carrying the AHC Torch
So here’s the million-dollar question: where does the Accountable Health Communities model go from here?
Accountable Care Organizations (ACOs) are stepping up to answer that call. These organizations already operate under value-based payment models that reward better outcomes, not just more services. That makes them natural allies in the push to integrate social care into healthcare delivery (Naeem et al., 2022).
But to pull it off, ACOs need to:
- Understand the real social needs of their populations
- Engage patients consistently across touchpoints
- Work closely with community-based organizations (CBOs)
- Track what’s working and what isn’t in real time
What’s stopping most ACOs? Outdated tools, disconnected systems, and staff stretched too thin. That’s where the right digital health platform can make or break success.
How the Calcium Platform Helps ACOs Operationalize AHC Insights
Enter Calcium. The Calcium digital health platform was practically built for moments like this. It’s a three-part system that helps both patients and providers stay connected, informed and engaged especially when it comes to addressing complex health-related social needs.
Let’s walk through how Calcium solves some of the biggest pain points exposed by the Accountable Health Communities model.
A. Real-Time Data Integration
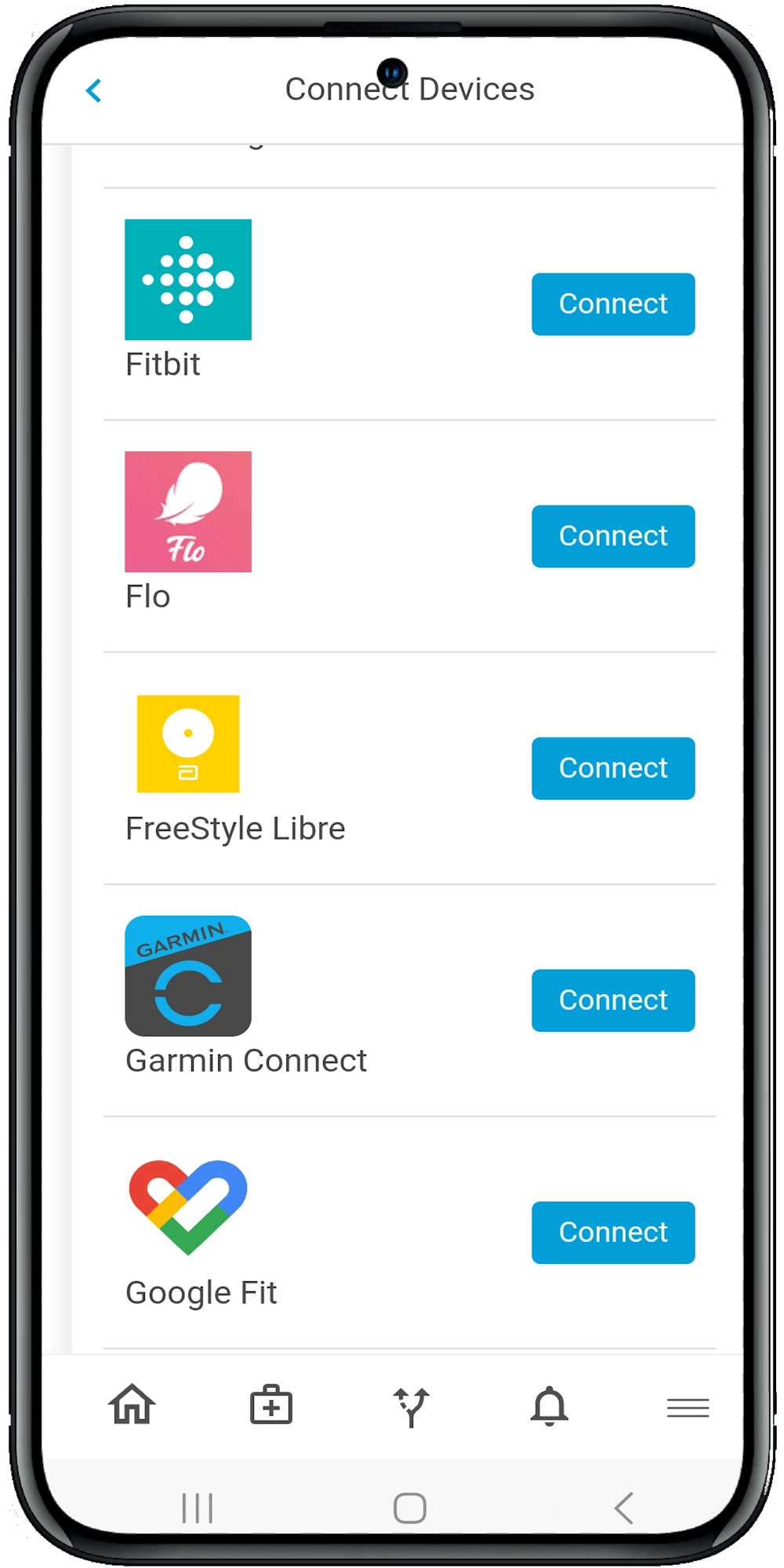
With Calcium, data isn’t trapped in silos. The platform integrates:
- Electronic Health Records (EHRs) from 95% of U.S. health systems
- Wearables like Apple Watch or Fitbit
- Smart medical devices like blood pressure cuffs and glucose monitors
- Social and behavioral health data from patient inputs
This gives providers and care teams a full 360-degree view of the patient not just the clinical snapshot. For ACOs, that’s pure gold.
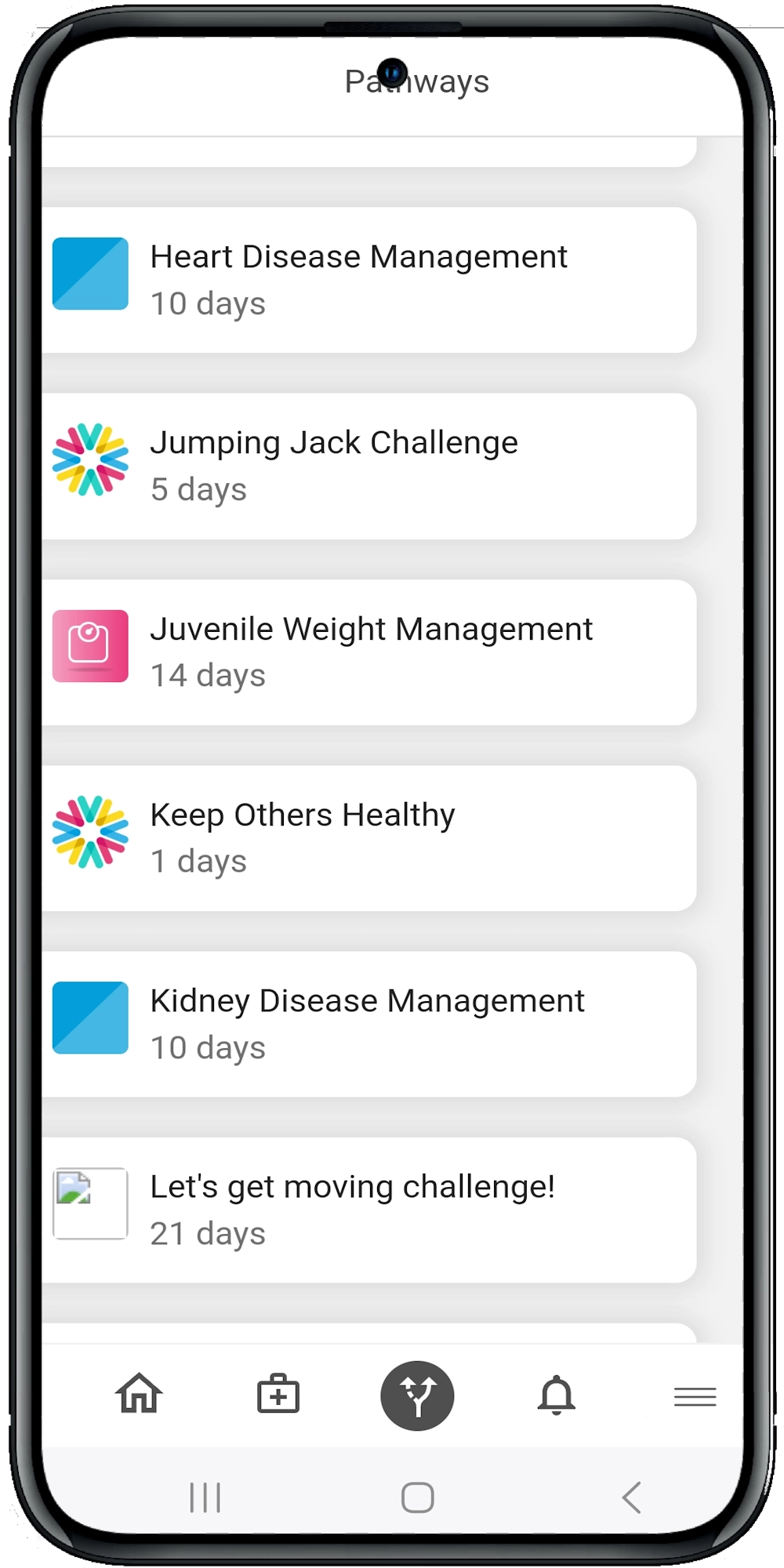
B. Personalized, AI-Powered Pathways
The Calcium Super App provides digital “pathways” step-by-step care plans that patients can follow at home. These can be tailored to:
- Food insecurity
- Chronic condition management
- Transportation needs
- Behavioral health or mental health support
Even better? These pathways use AI to adapt over time based on patient input and progress. This means each patient’s journey is dynamic, not one-size-fits-all.
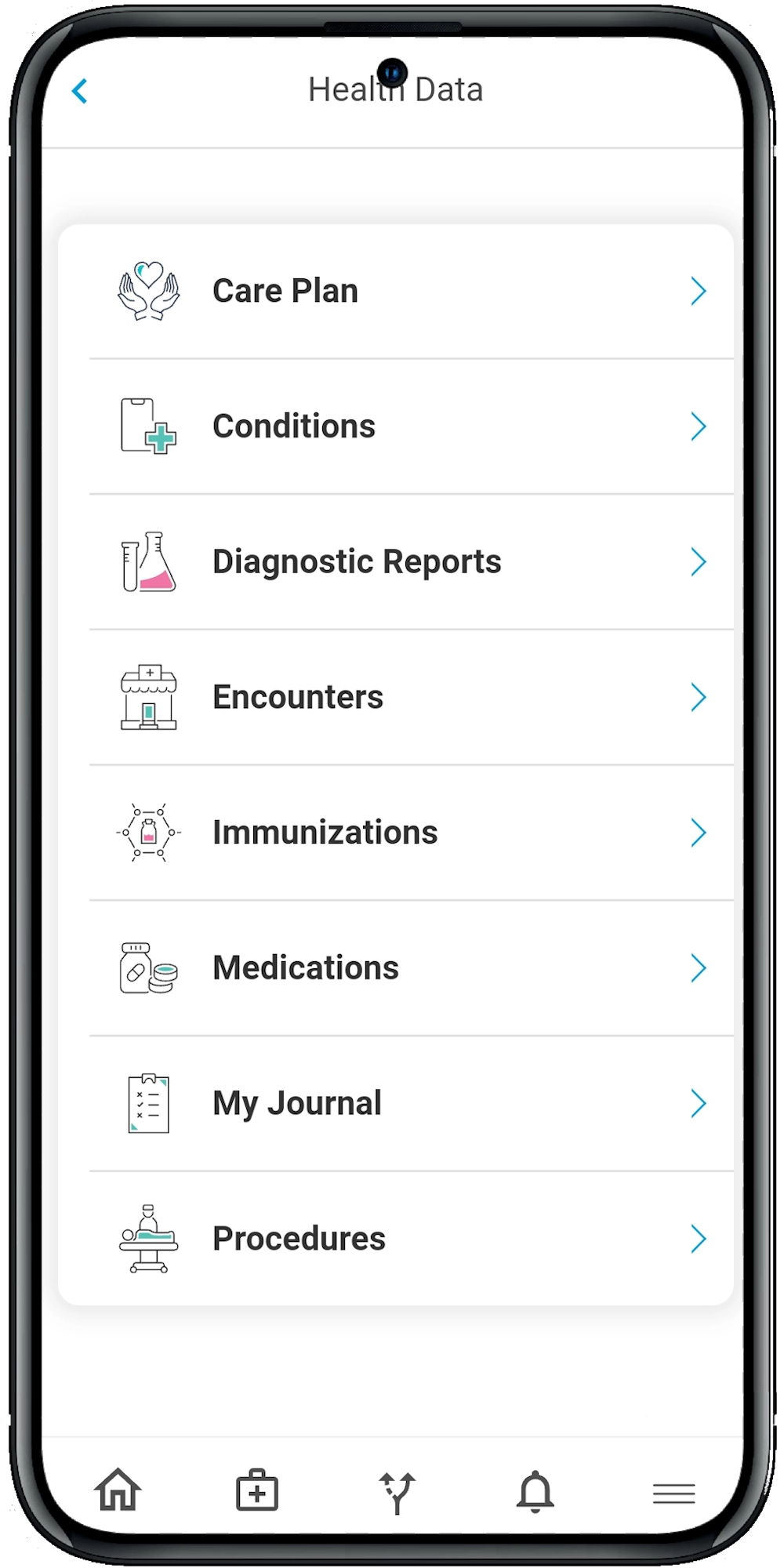
C. Constant Engagement Through the Super App
The Super App is like having a digital health coach in your pocket. Patients can:
- Log symptoms in their health journal
- Receive medication reminders
- Track vitals automatically
- Share updates with their provider team
This kind of consistent, low-friction engagement is what the AHC model was missing. And it makes a big difference in improving outcomes—especially for hard-to-reach populations.
D. Closed-Loop Referrals and Accountability
Calcium’s Core dashboard allows providers to assign pathways, track completion, monitor alerts, and see unresolved referrals. This creates the feedback loop that the original AHC efforts lacked (Renaud et al., 2023).
Plus, providers get real-time analytics on which interventions are working and which patients need extra help. This helps ACOs prioritize care, allocate resources smartly, and actually measure the ROI of their social care investments.
E. Scalable Navigation Support
Instead of hiring armies of overburdened navigators, ACOs can use Calcium to automate many common touchpoints:
- Appointment reminders
- Follow-ups after hospital discharge
- Progress checks within care pathways
This doesn’t eliminate the need for human navigators, it amplifies their impact.
The Future Is Whole-Person Care
The Accountable Health Communities model was a big step in the right direction. It validated what we’ve always known: people’s health is shaped just as much by their environment as by their prescriptions (Johnson et al., 2022). But good intentions alone aren’t enough. We need technology that makes whole-person care scalable, measurable, and sustainable.
That’s where ACOs come in and with the help of platforms like Calcium, they’re in a strong position to take what the AHC model started and bring it to life at scale.
The Wrap
The Accountable Health Communities model showed us what’s possible when we start treating social needs as clinical priorities but it also revealed just how complex that mission can be. Real change takes more than good ideas. It takes tools that connect people, data, and care in real time. It takes platforms that don’t just track progress but help drive it. That’s exactly where ACOs have the opportunity to lead and where Calcium can help.
With our AI-powered Super App and provider-facing Core platform, we’re making it easier to identify, track, and resolve the real-life barriers your patients face every day. Whether you’re managing chronic conditions, coordinating with community partners, or scaling whole-person care across your network, Calcium gives you the digital backbone to do it smarter.
Reference
- Parish, W. J., Beil, H., He, F., D’Arcangelo, N., Romaire, M., Lucia Rojas Smith, & Haber, S. (2023). Health Care Impacts Of Resource Navigation For Health-Related Social Needs In The Accountable Health Communities Model. Health Affairs, 42(6), 822–831. https://doi.org/10.1377/hlthaff.2022.01502
- Johnson, K. A., Barolin, N., Ogbue, C., & Verlander, K. (2022). Lessons From Five Years Of The CMS Accountable Health Communities Model. Health Affairs Forefront. https://www.healthaffairs.org/content/forefront/lessons-five-years-cms-accountable-health-communities-model
- Naeem, J., Salazar-Contreras, E., Sundaram, V., Wainwright, L., Kosel, K., & Miff, S. (2022). The Dallas Accountable Health Community: Its Impact on Health-Related Social Needs, Care, and Costs. NEJM Catalyst, 3(9). https://doi.org/10.1056/cat.22.0149
- Renaud, J., McClellan, S. R., DePriest, K., Witgert, K., O’Connor, S., Kate Abowd Johnson, Barolin, N., Gottlieb, L. M., De, E. H., Rojas-Smith, L., & Haber, S. G. (2023). Addressing health-related social needs via community resources: Lessons from accountable health communities. Health Affairs, 42(6), 832–840. https://doi.org/10.1377/hlthaff.2022.01507