Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
Transforming Reactive Care into a Proactive Accountable Care Strategy
In value-based care, success isn’t just about delivering care — it’s about delivering the right care to the right patients at the right time. For Accountable Care Organizations (ACOs), that means prioritizing limited resources for the people who need them most.
But how do you know who those people are before they fall through the cracks? That’s where risk stratification becomes critical. In theory, it’s the secret weapon for proactive care management.
In practice, though, many ACOs are still using outdated or incomplete tools that don’t reflect the complexity of real lives or real-time data. As patient needs grow more diverse — and care becomes more data-driven — the stakes have never been higher. If your ACO is still using the same risk models from five years ago, it’s time to rethink the foundation of your population health strategy. Because in today’s healthcare environment, precision isn’t optional — it’s essential.
Why ACOs Rely on Risk Stratification — and Where It Falls Short
Let’s be honest — ACOs have one of the toughest balancing acts in healthcare. They need to lower costs while keeping patients healthier and providers satisfied. Risk stratification helps make that possible by separating patients into different risk levels based on health status, utilization history, and sometimes, social factors.
But here’s the catch: most ACO risk stratification tools were built for yesterday’s problems. They often rely on old claims data, overlook behavioral or social risks, and struggle to pinpoint which patients are about to become high-cost, not just those who already are.
That’s like trying to predict a traffic jam by looking at last month’s GPS logs.
Common Problems with Traditional ACO Risk Stratification Tools
Before diving into solutions, let’s walk through the core issues that still plague many ACOs using legacy tools.
1. Outdated Data Means Delayed Action
Claims-based tools like CMS-HCC and DxCG are commonly used. While they’re decent at identifying current high utilizers, they’re built on retrospective data — which often lags by 3 to 6 months. In fast-moving clinical situations, that’s a lifetime.
Imagine trying to intercept a patient’s downward health spiral after the fact. Too late. By the time the alert shows up, the avoidable ER visit or hospitalization already happened (Haas et al., 2013).
2. Missing the Whole Picture
Let’s face it — healthcare doesn’t happen in a vacuum. Things like food insecurity, housing instability, stress, and behavioral health all influence outcomes. Yet most ACO risk stratification tools don’t consider these social determinants of health (SDOH).
AI models that incorporate ADT alerts and SDOH data have been shown to significantly outperform traditional tools in predicting which patients would incur the highest future costs (Carroll et al., 2022).
3. Rising-Risk Patients Get Overlooked
Most tools are really good at telling you who’s already sick. But what about those who are just starting to decline?
These are the patients who don’t yet look expensive but will be soon. If you wait until they show up in your “top 5% spend” reports, you’ve already missed your window.
ACO leaders have emphasized the importance of segmentation—dividing high-need, high-cost populations into meaningful subgroups to guide interventions. That’s tough to do with flat, rule-based models (O’Malley et al., 2019).
4. Limited Personalization for Diverse Populations
Here’s the reality: a 75-year-old patient with congestive heart failure shouldn’t be risk-stratified using the same model as a 12-year-old with uncontrolled asthma. But many systems try to do just that.
Deep learning models have demonstrated superior performance in predicting hospitalization risk among pediatric ACO patients compared to traditional methods, highlighting the need for more tailored approaches (Lin et al., 2019).
The Rise of AI-Powered, Real-Time Risk Stratification
So what’s the fix? The future of ACO risk stratification tools lies in blending the old with the new — integrating proven clinical data models with real-time, AI-powered analytics and digital engagement.
Here’s what leading-edge risk stratification looks like:
1. Multisource Data Fusion
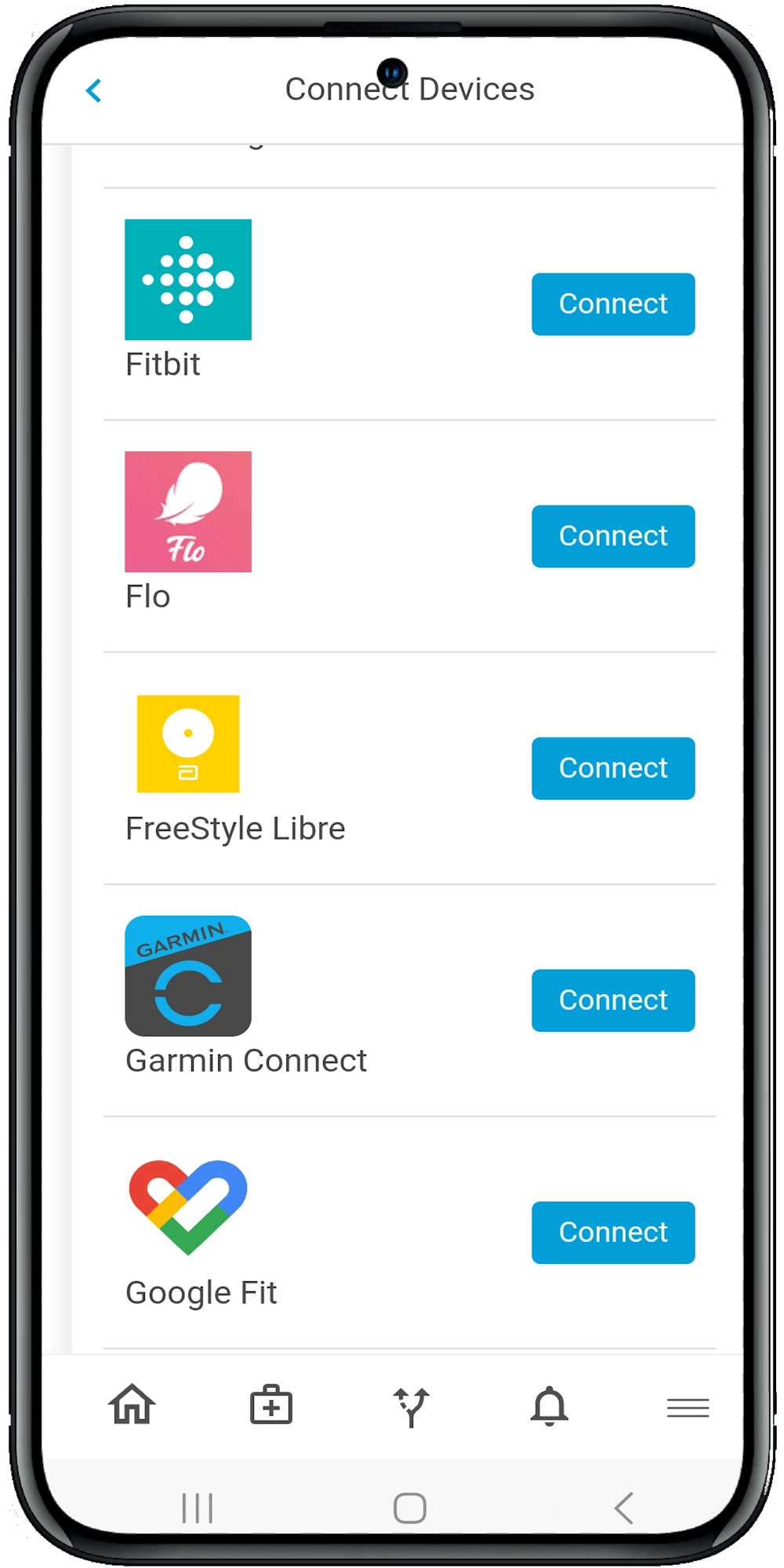
Newer tools don’t just rely on claims. They pull from:
- Real-time ADT feeds
- SDOH assessments
- Health surveys
- Wearables and device data
- EHR and medication adherence logs
Think of it like going from a grainy black-and-white photo to a 4K health portrait. You’re no longer guessing who’s at risk — you can see it unfold in real time (Carroll et al., 2022).
2. Deep Learning Models That Adapt Over Time
Rather than using static scoring models, AI-driven systems can learn patterns, identify anomalies, and adjust as patient behavior changes.
For example, a deep learning model used in a pediatric ACO setting identified 41% more high-cost patients than traditional tools, with those patients incurring $5 million more in actual spend (Lin et al., 2019). That’s the kind of insight that changes how ACOs plan and prioritize.
3. Predictive & Preventive, Not Just Reactive
By combining AI models with early symptom tracking, remote monitoring, and care team alerts, the best tools now help ACOs prevent hospitalizations instead of simply predicting them.
It’s like having an early-warning system for patient decline — and the ability to respond before it turns into a crisis.
Bridging the Gap: How Calcium Elevates Risk Stratification for ACOs
At this point, it’s clear that most ACO risk stratification tools need an upgrade. That’s where platforms like Calcium come in.
Here’s how Calcium transforms patient prioritization in ACO settings:
1. Real-Time Risk Scoring + Digital Engagement
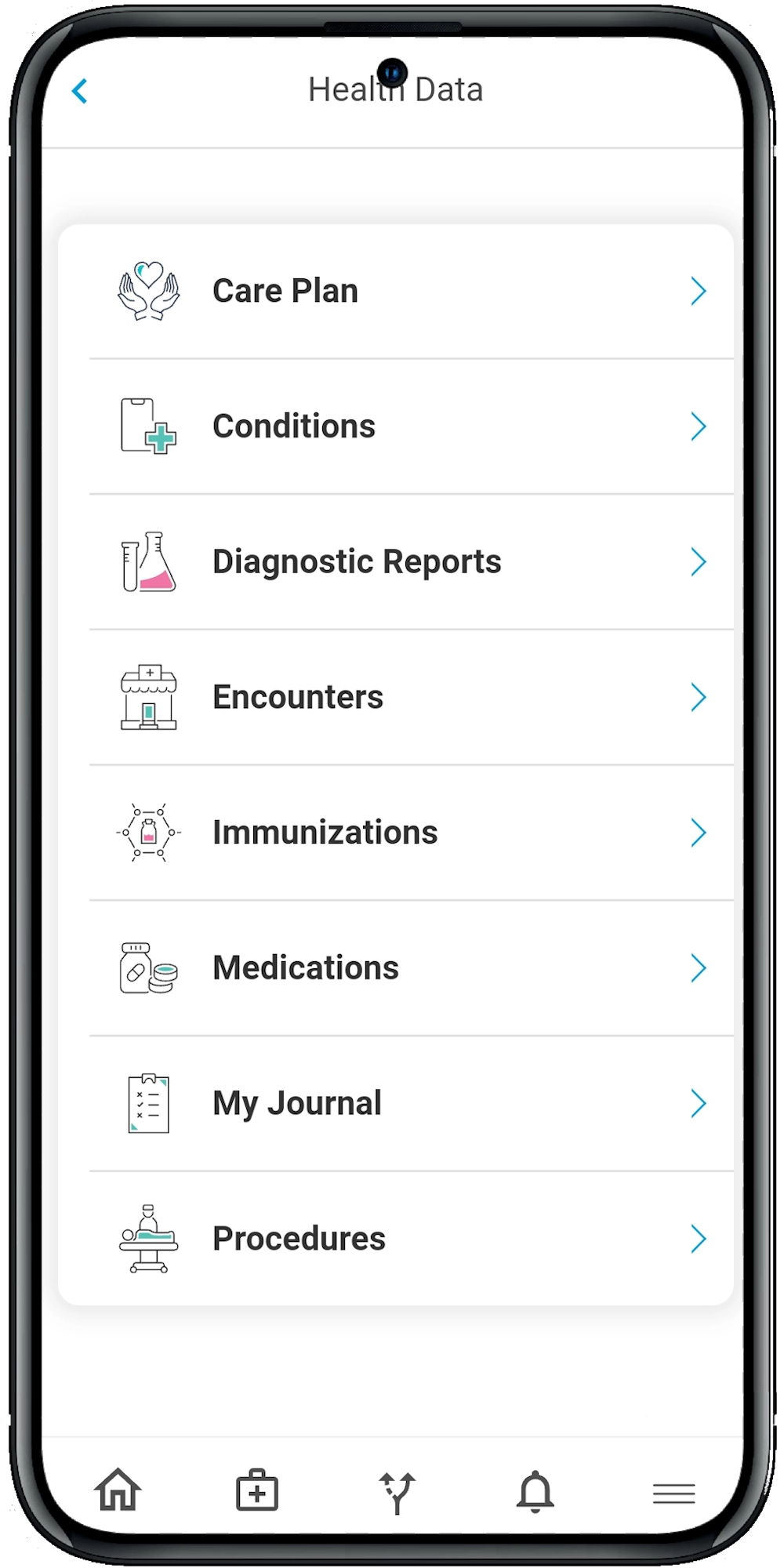
Calcium doesn’t just assign a risk score and walk away. It uses real-time inputs — like vital signs from devices, medication tracking, and health journal entries — to continuously reassess patient risk and flag concerns.
So if a diabetic patient skips meds for three days or logs high blood sugar in their journal, that risk score updates immediately — and care teams can intervene.
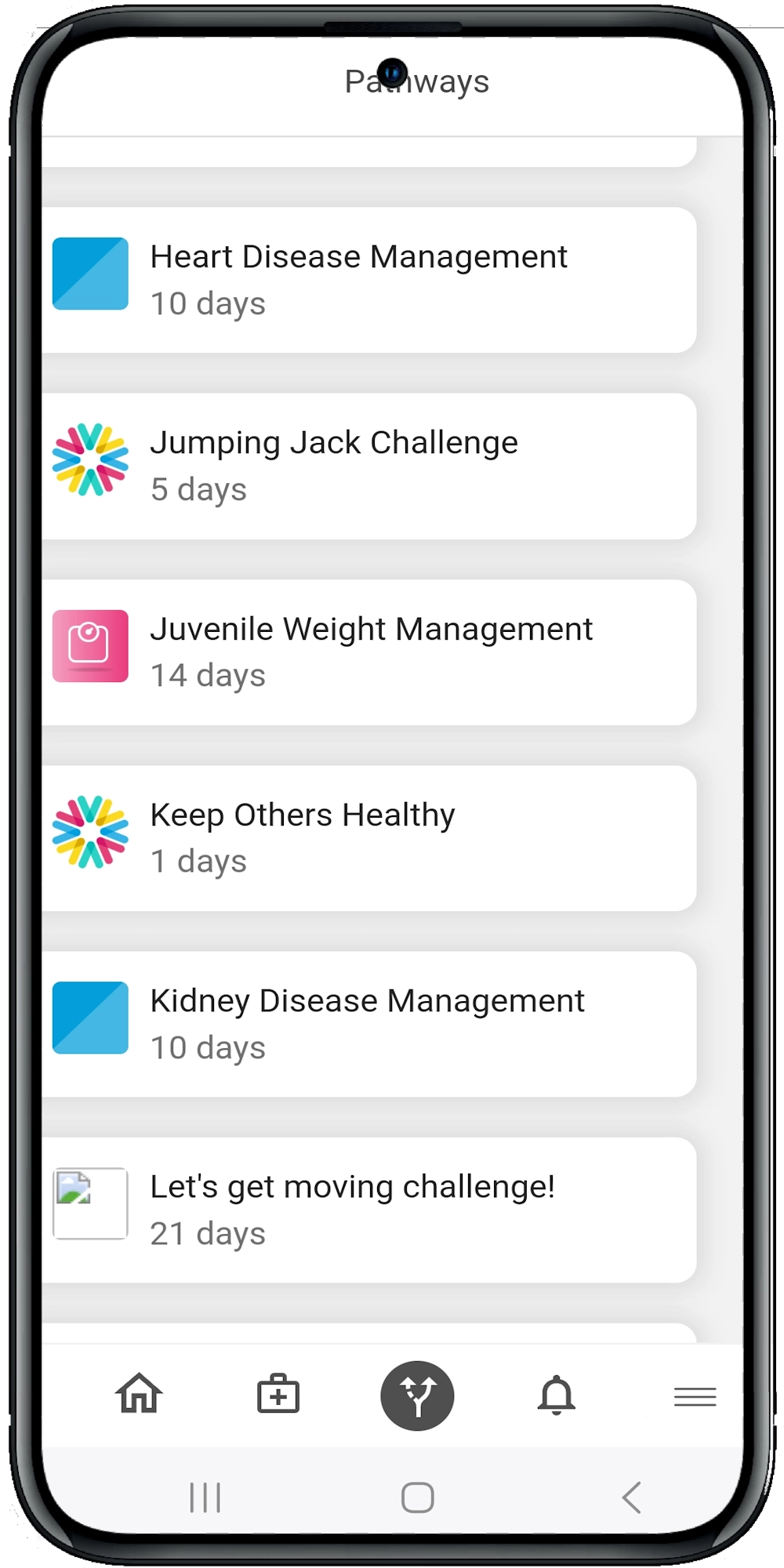
2. Actionable Pathways, Not Just Alerts
Risk alerts mean little if there’s no plan. Calcium’s Super App pairs risk scores with digital health pathways that guide the patient through their condition — whether it’s hypertension, post-surgical care, or depression.
These aren’t static checklists. They include:
- Daily reminders
- Health education
- Progress tracking
- Behavior nudges
- Care team messaging
It’s like giving every patient their own personalized GPS — with their provider watching the route in real time.
3. Support for Behavioral and Social Health
Mental health is often ignored in traditional stratification. Calcium integrates behavioral pathways for anxiety, ADHD, addiction recovery and more — along with prompts to assess SDOH like food access or transportation barriers.
That’s crucial for ACOs working with Medicaid populations, where behavioral health and social needs drive much of the cost and risk (Carroll et al., 2022).
4. Closed-Loop Feedback to Improve Accuracy
The Calcium platform doesn’t just assign pathways — it measures how well they work. By tracking pathway completion, symptom changes and utilization outcomes, ACOs can refine their risk models over time.
You’re not just predicting risk — you’re validating it against real-world results.
5. Designed for Whole-Person Care, Not Just Metrics
One of the biggest differences with Calcium is that it’s built to treat people — not just populations. While traditional ACO risk stratification tools focus on checkboxes and cost curves, it centers the entire experience around the patient’s goals, habits, and lifestyle.
It allows for:
- Patient journaling and symptom check-ins
- Family and caregiver involvement
- Custom alerts based on patient behavior
- Bi-directional communication between patients and care teams
This approach brings humanity back into the care equation. Because when you give people tools they can actually use — on their phones, in their own words, in real time — you stop treating them like risk scores and start treating them like partners in their own care.
The Wrap
Risk stratification is no longer a nice-to-have for ACOs — it’s a must. But to truly make an impact, today’s tools need to go beyond outdated claims data and static risk scores. They must be intelligent, real-time, and deeply connected to the patient experience.
That’s where platforms like Calcium come in. By combining AI-powered insights, digital care pathways, behavioral health support, and real-time engagement, Calcium helps ACOs not only identify who’s at risk but take meaningful action before it’s too late. Whether you’re trying to lower costs, boost outcomes, or better serve high-need populations, smarter risk stratification is the starting point.
Reference
- Carroll, N., Jones, A., Burkard, T., Lulias, C., Severson, K., & Posa, T. (2022). Improving Risk Stratification Using AI and Social Determinants of Health. (2022). The American Journal of Managed Care, 28(11), 582–587. https://doi.org/10.37765/ajmc.2022.89261
- Lindsey R. Haas, M. P. H., Paul Y. Takahashi, M. D., Nilay D. Shah, P., Robert J. Stroebel, M. D., Matthew E. Bernard, M. D., Dawn M. Finnie, M. P. A., & James M. Naessens, S. (2013). Risk-Stratification Methods for Identifying Patients for Care Coordination. Www.ajmc.com, 19. https://www.ajmc.com/view/risk-stratification-methods-for-identifying-patients-for-care-coordination
- Lin, E.-J., Hefner, J., Zeng, X., Moosavinasab, S., Huber, T., Klima, J., Liu, C., & Lin, S. (n.d.). A Deep Learning Model for Pediatric Patient Risk Stratification. Retrieved May 30, 2025, from https://ajmc.s3.amazonaws.com/_media/_pdf/AJMC_10_2019_Lin%20final.pdf
- Coran, J. J., Schario, M. E., & Pronovost, P. J. (2021). Stratifying for Value: An Updated Population Health Risk Stratification Approach. Population Health Management. https://doi.org/10.1089/pop.2021.0096
- O’Malley, A. S., Rich, E. C., Sarwar, R., Schultz, E., Warren, W. C., Shah, T., & Abrams, M. K. (2019). How Accountable Care Organizations Use Population Segmentation to Care for High-Need, High-Cost Patients. Issue Brief (Commonwealth Fund), 2019, 1–17. https://pubmed.ncbi.nlm.nih.gov/30645057/