Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
Coordinating care at scale demands purpose-built digital tools—not just good intentions or more staffing
In value-based care (VBC), you’re rewarded for outcomes, not just activity. But when your population includes patients with cancer, multiple chronic conditions, behavioral health needs, or significant social barriers, coordinating care isn’t just difficult—it’s high stakes.
For teams managing these complex patients, care plans often cross multiple specialties, systems, and locations. There’s no room for communication gaps, dropped tasks, or delayed follow-ups. Yet without the right tools, that’s exactly what happens. The truth? Most health systems are still relying on manual processes, siloed data, and fragmented platforms to manage incredibly complicated care journeys.
It’s no wonder care teams burn out, patients fall through the cracks, and outcomes suffer.
What Makes a VBC Population Complex?
It’s not just about the clinical diagnosis. Complexity in VBC means a mix of challenges that make coordination harder and more critical. Think about:
- Cancer patients seeing multiple specialists while undergoing chemo
- Diabetic patients with depression and food insecurity
- Children with rare conditions managed by a team across hospital, home, and community providers
These aren’t outliers—they’re becoming the norm. And as the healthcare system shifts toward accountability for whole-person outcomes, the pressure to manage these cases effectively keeps rising.
The key? Stop trying to do it all manually. Instead, equip your team with tools designed to support integrated, real-time collaboration.
Where Coordination Breaks Down
The first step in solving care coordination issues is understanding where they come from. Across multiple studies—including the Systematic Review of Care Coordination Models—the problems are shockingly consistent.
Here are the most common failure points:
- Lack of shared care plans. Everyone’s operating from different playbooks.
- Unclear roles. No one knows who’s in charge of what, especially across sites or systems.
- Fragmented communication. Important updates get lost between inboxes, calls, and sticky notes.
- Manual follow-ups. Staff track transitions and tasks with spreadsheets and emails.
- Poor measurement. Coordination success isn’t visible or measured well.
This creates friction for everyone involved—and delays for patients who don’t have time to wait.
The Tools Your Care Team Actually Needs
If you’re serious about coordinating complex VBC populations, you need more than a messaging system or EHR add-on. You need a digital infrastructure built for proactive, team-based care.
Here are the essential tools that make that possible:
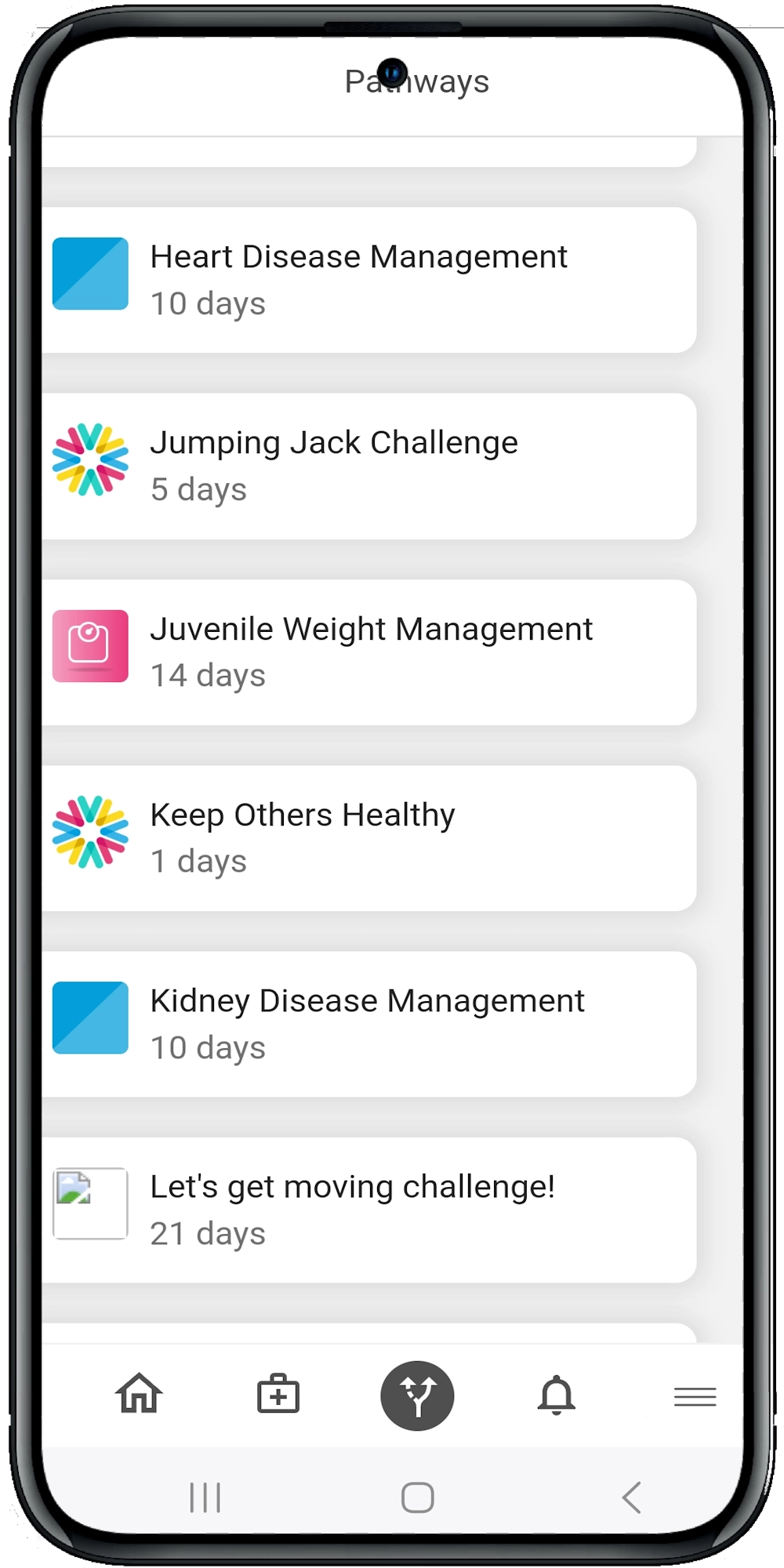
1. Shared Digital Care Pathways
Instead of disconnected care plans in separate systems, use digital pathways that follow the patient across specialties and care settings.
These pathways should be:
- Pre-built for conditions like cancer, diabetes, or CHF
- Customizable per patient based on comorbidities or social needs
- Visible to every provider, care manager, and family member involved
- Triggered by real-time data (e.g., new lab result or missed appointment)
The Care Coordination Models review emphasized that shared care plans drive consistency and reduce duplicative services—especially when tools support updates in real time.
2. Role-Based Task Assignment and Alerts
Care isn’t delivered by one person. It’s a team sport.
That’s why you need tools that assign, route, and escalate tasks across disciplines. Your platform should:
- Let team members assign follow-ups or outreach tasks
- Send alerts if a high-risk patient misses a milestone
- Provide role-specific dashboards for nurses, social workers, and pharmacists
- Log who did what and when—creating accountability and clarity
Without this, your team ends up duplicating efforts or letting critical handoffs fall through.
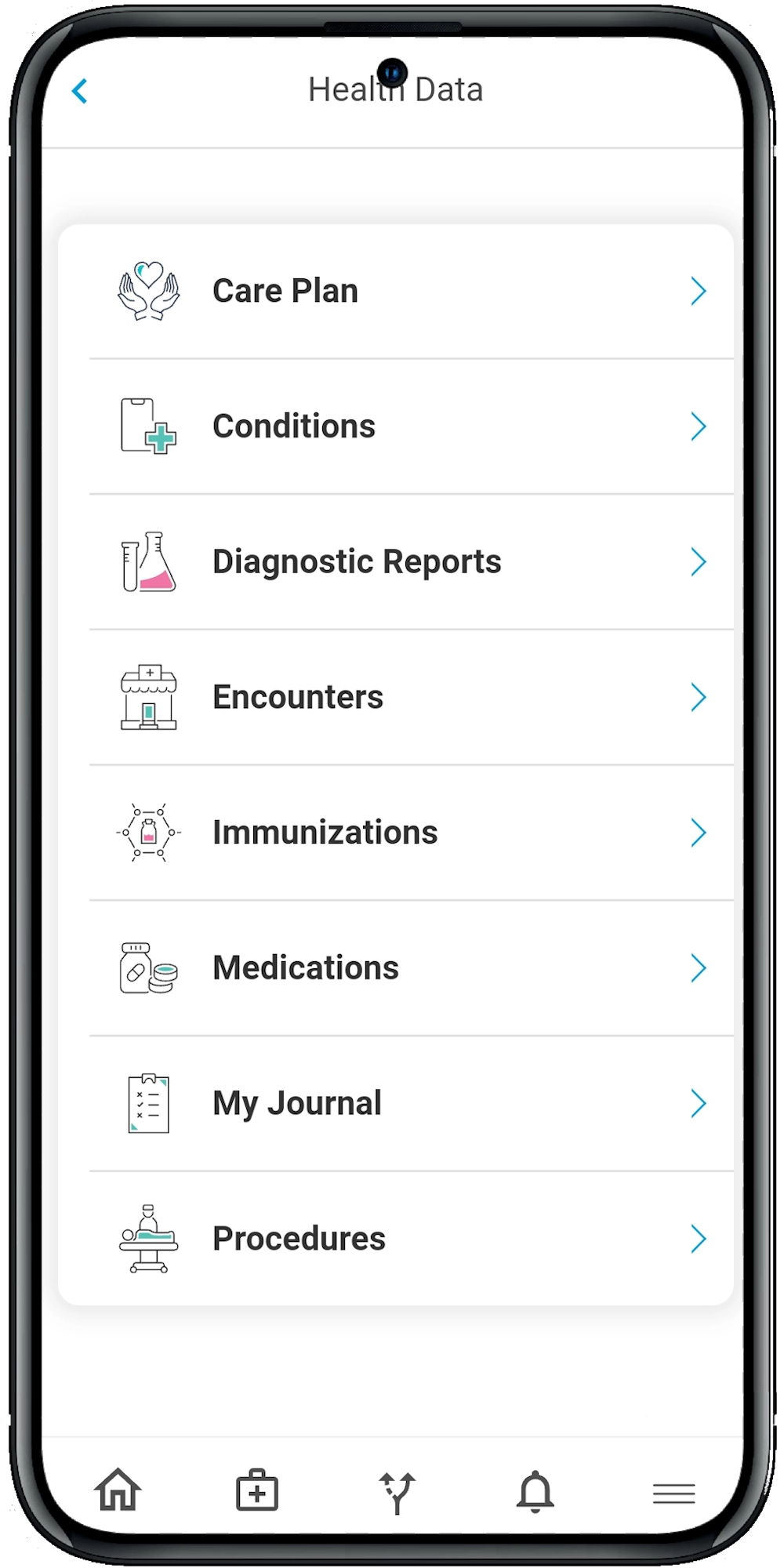
3. Engagement Tools for Patients and Caregivers
Don’t underestimate the power of the patient-facing side. Especially in oncology or chronic care, patients and caregivers play a huge role in day-to-day success.
Give them:
- Mobile access to care plans, reminders, and education
- A way to journal symptoms, mood, or side effects
- Push notifications for medications or appointments
- Shared access so family members or caregivers can stay in the loop
The Care Coordination for Children with Medical Complexity study revealed how unclear roles between families and care teams create stress and confusion. Transparent tools solve that.
4. AI-Powered Risk Stratification and Dynamic Prioritization
Not all patients need the same intensity of outreach every day. AI-driven platforms help teams focus by automatically:
- Flagging rising-risk patients based on symptoms or missed steps
- Adjusting care plan urgency based on clinical data or SDOH
- Prioritizing outreach based on impact potential and risk
It’s like giving your care managers a radar system instead of making them scan the horizon manually.
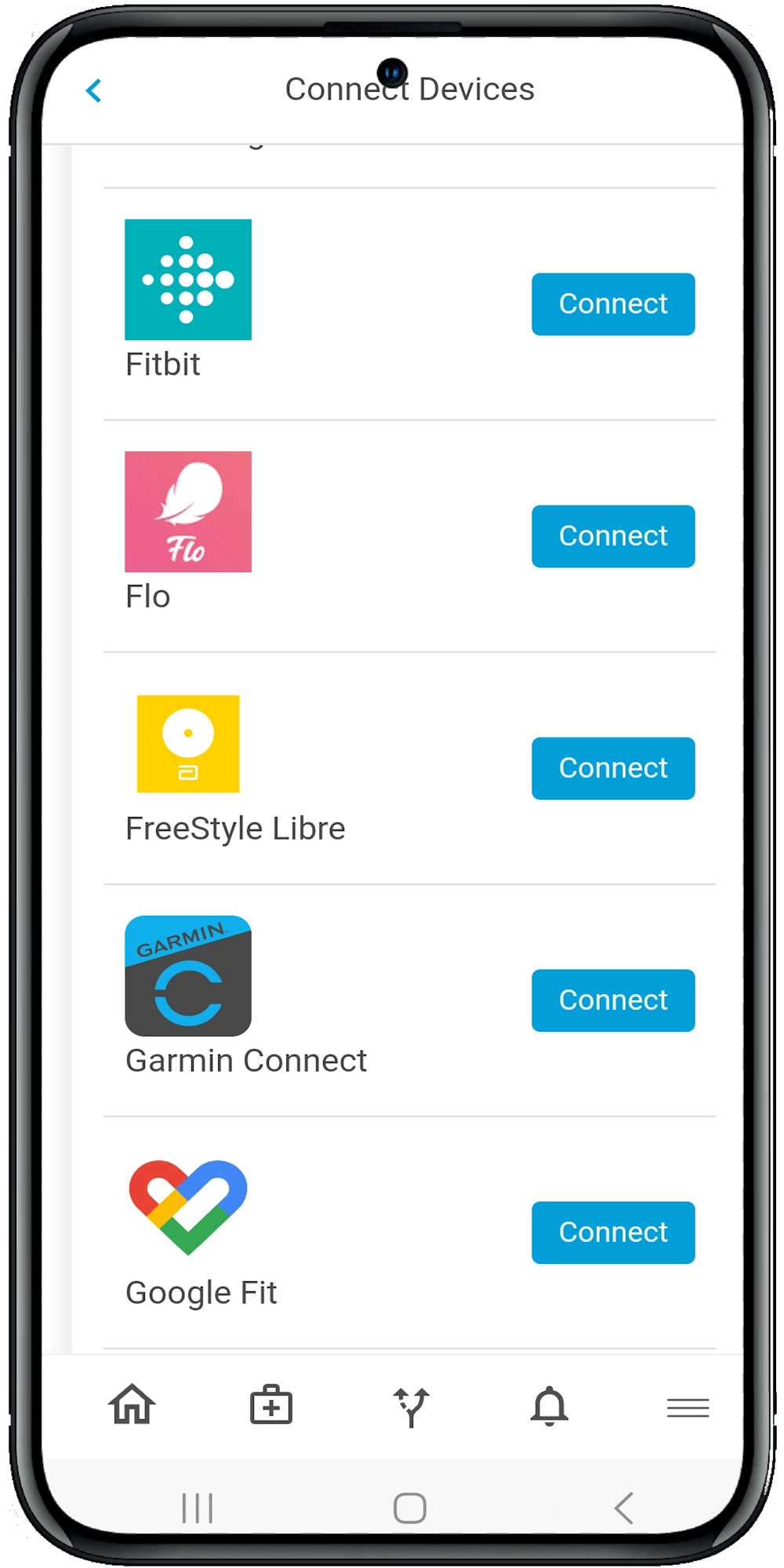
5. A Communication Hub That Spans Systems
Care integration fails when information stays trapped inside one system or team.
Your coordination platform should offer:
- Secure team messaging across provider groups
- Structured communication prompts (e.g., “lab pending” or “discharge follow-up needed”)
- Integration with EHRs, labs, and community platforms
- A searchable audit trail of communication across the care continuum
The Moving from Care Coordination to Care Integration paper makes it clear: real progress comes when systems talk to each other and workflows operate across organizations—not just within them.
6. Real-Time Metrics and Coordination KPIs
You can’t improve what you don’t measure. Robust digital platforms give you access to:
- Care pathway adherence rates
- Time-to-follow-up after discharge
- Preventable ED visits or readmissions
- Task completion rates across roles
- Patient-reported engagement and satisfaction
The Systematic Review of Care Coordination Measurement found that current evaluation tools are too inconsistent. Digital platforms can fill that gap with consistent, automated tracking.
Why Manual Doesn’t Scale—And Digital Does
Trying to coordinate complex care without the right tools is like trying to fly a plane with a paper map and walkie-talkies. It might work on a clear day with one or two passengers—but scale it up, add turbulence, and things fall apart fast.
Digital platforms—especially those built for VBC—offer the infrastructure your team needs to:
- Keep everyone on the same page
- Focus effort where it matters most
- Empower patients and families
- Report what’s working and what’s not
And most importantly, they help care teams spend less time chasing down tasks and more time actually caring for people.
The Wrap
Coordinating care across complex populations isn’t just about keeping up—it’s about staying ahead. When your team is managing patients with chronic conditions, cancer, behavioral health needs, and social risk factors, the right tools can make the difference between fragmentation and fluidity, between missed opportunities and measurable impact.
You don’t need more spreadsheets, phone calls, or siloed portals. You need a platform that connects the dots in real time, empowers your team, and keeps patients actively engaged in their care journey.
That’s exactly what the Calcium digital health platform was built to do. From shared care pathways to AI-powered task management, from patient engagement to real-time analytics, Calcium gives your team the infrastructure to thrive in today’s value-based world.
Reference
- Duan-Porter, W., Ullman, K., Majeski, B., Miake-Lye, I., Diem, S., & Wilt, T. J. (2021). Care Coordination Models and Tools—Systematic Review and Key Informant Interviews. Journal of General Internal Medicine, 37(6), 1367–1379. https://doi.org/10.1007/s11606-021-07158-w
- Schultz, E. M., Pineda, N., Lonhart, J., Davies, S. M., & McDonald, K. M. (2013). A systematic review of the care coordination measurement landscape. BMC Health Services Research, 13(1). https://doi.org/10.1186/1472-6963-13-119
- Kuo, D., McAllister, J., Rossignol, L., Turchi, R., & Stille, C. (2022). Care Coordination for Children With Medical Complexity: Whose Care Is It, Anyway? Pediatrics – American Association of Pediatrics. https://publications.aap.org/pediatrics/article/141/Supplement_3/S224/34444/Care-Coordination-for-Children-With-Medical
- Poku, M. K., Kagan, C. M., & Yehia, B. (2019). Moving from Care Coordination to Care Integration. Journal of General Internal Medicine, 34(9), 1906–1909. https://doi.org/10.1007/s11606-019-05029-z