Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
Closing the Gaps in Care with Smarter, Real-Time Medication Tracking and Patient-Centered Tools
What if a single missing medication record could mean the difference between recovery and readmission or worse? In today’s complex healthcare environment, clinicians don’t just need data; they need the right data at the right time.
Yet too often, a patient’s medication history is incomplete, outdated or buried in a digital maze of disconnected systems. From emergency departments to primary care clinics, the consequences are real: missed drug interactions, medication errors and fragmented care. As we shift toward value-based models and personalized treatment, accessing an accurate and comprehensive medication history isn’t a luxury it’s a necessity.
But why is it still so hard? And more importantly, what can we do about it? The answer lies in smarter, patient-centered platforms that bridge the gaps traditional EHRs leave behind.
Why Medication History Matters More Than Ever
Imagine walking into an ER, unable to remember the name of your blood pressure medication let alone the dosage or when you last took it. Now multiply that across thousands of patients every day. That’s the challenge facing providers who lack access to a complete patient medication history.
Accurate medication records are the bedrock of safe, coordinated, and effective care. Whether a patient is being seen for chronic disease management, pre-op clearance or an unexpected ER visit, knowing what medications they’re on (and actually taking) can make or break clinical outcomes.
In today’s value-based care landscape, where quality and efficiency are non-negotiable, incomplete or fragmented medication history isn’t just a documentation issue it’s a patient safety risk.
Real-World Challenges with Medication History in EHRs
Despite all the progress in digital health, many EHRs still fall short when it comes to medication records. Here are the top challenges providers and patients run into:
1. Fragmented Records Across Systems
It’s common for patients to see multiple providers a primary care doctor, a few specialists, maybe a mental health counselor. But if those providers use different EHR platforms, medication records can get stuck in separate silos.
As Kalra’s research points out, structural incompatibilities between EHRs make data sharing difficult and strip clinical context during transfers. This turns dynamic health histories into static documents.
2. Missing Data from Pharmacies and OTC Meds
Pharmacy data doesn’t always flow into EHRs. Even worse, over-the-counter medications, vitamins, and supplements rarely get recorded unless the patient remembers to mention them.
That’s a big problem. These medications may interact with prescriptions or affect lab results, but they’re often invisible to clinicians making decisions in the moment.
3. Patient Memory Isn’t Reliable
Let’s be honest most of us can’t recite the names, doses, and schedules of every medication we’ve taken in the past year. For patients on multiple meds, especially older adults, it’s even harder.
Relying on verbal self-reporting during a 10-minute office visit is like asking someone to remember every stop on a road trip without a map.
4. Clunky EHR Interfaces Hide Key Info
Ambinder’s study of oncology EHRs showed that even when medication data was present, it was hard to find or interpret. Poor design makes it difficult to see dosing schedules, refill history, or medication changes over time.
When information is buried in tabs or buried in notes, it may as well not exist. Usability isn’t a luxury it’s a necessity.
5. No Real-Time Adherence Data
Just because a medication was prescribed doesn’t mean it’s being taken. Most EHRs can’t track whether a patient actually picked up their prescription or followed through on refills.
That’s a critical blind spot in chronic condition management especially for conditions like diabetes, hypertension, or depression where missed doses can spiral into complications.
6. Lack of Clinical Context
It’s not enough to see what meds a patient is on providers need to understand why they were prescribed, how long ago, and whether they were effective or discontinued.
Without that narrative, records are just static snapshots. As noted in the studies, EHRs often fail to preserve intent, chronology, or nuance all of which are essential for safe prescribing.
7. Manual Entry Wastes Time and Risks Errors
In many settings, providers or staff still enter medication histories by hand, pulling from faxes, patient printouts or memory. That’s time-consuming, error-prone, and not scalable.
If digital records can’t automatically capture and reconcile medication data, they become just another administrative burden.
What the Research Says: It’s Not Just the Tech — It’s the Design
All three studies behind this post agree: having digital records isn’t enough. For EHRs to truly support clinical decision-making, they need to be accurate, complete and intuitive.
One study found an impressive 99.7% accuracy rate in medication records but only when EHR systems were properly implemented, validated and supported by the right workflows and training. That’s not the norm across the industry.
Another key takeaway? Systems must balance standardization with flexibility. Medication modules need to be structured but still allow room for clinical notes, adjustments and decision reasoning. Otherwise, we risk turning clinicians into data-entry clerks rather than care providers.
Finally, all research emphasized one key truth: no digital record can replace human clinical judgment. But it should absolutely support it not get in the way.
How Calcium Fixes the Medication History Gap
This is where the Calcium digital health platform shines. Unlike traditional EHRs that focus on billing and documentation, Calcium is designed to support real-world care with real-time medication visibility for both providers and patients.
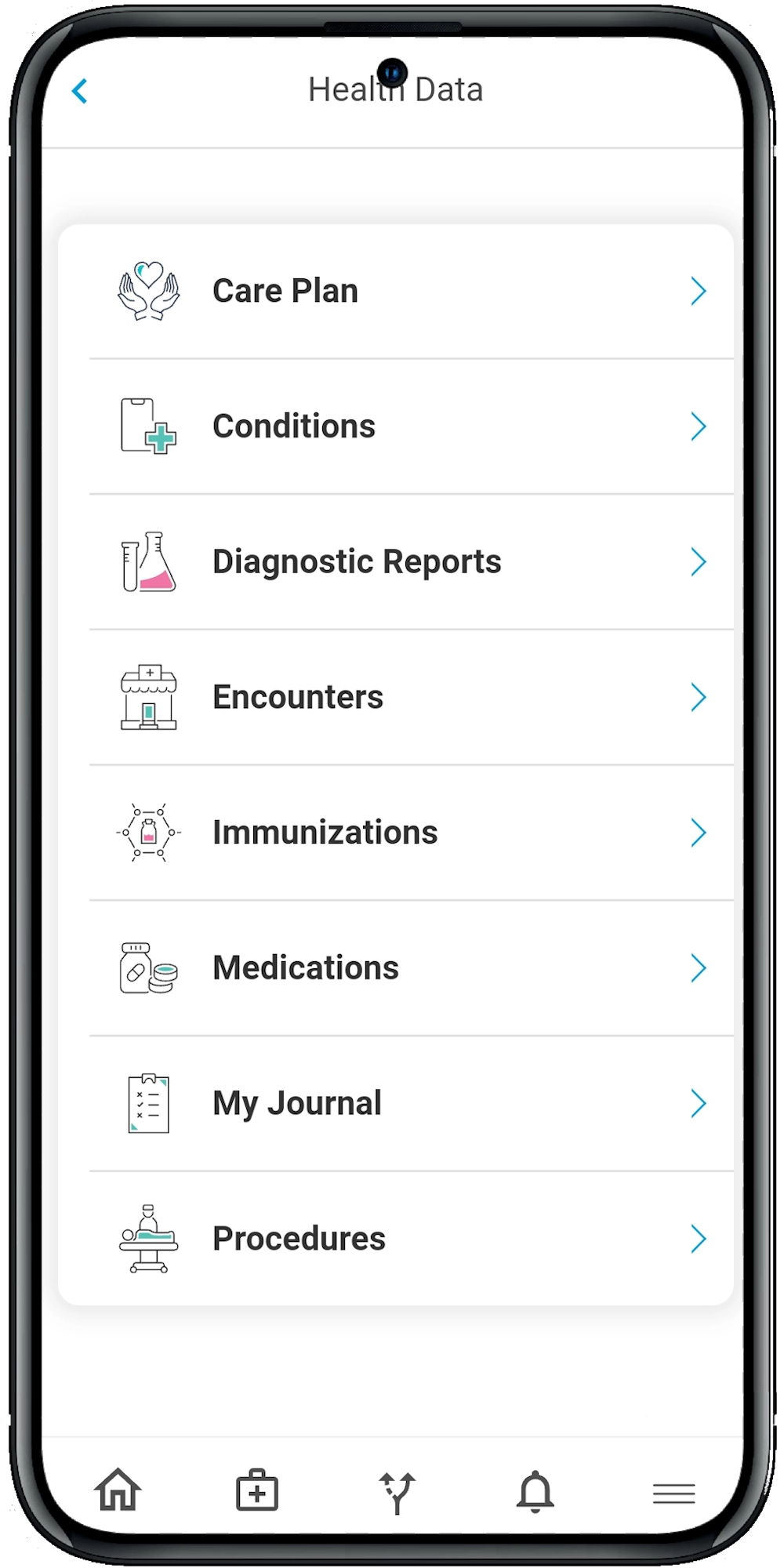
1. All-in-One View Through Calcium Core
Calcium Core, the provider-facing platform, consolidates data from 95% of U.S. health systems using national standards like HL7 and FHIR. That means:
- Medication data from hospitals, primary care, specialists and labs
- Reconciled lists that flag discrepancies or duplications
- Medication modules enriched with lab results, vitals and care plan context
No more jumping between systems or piecing together records from PDFs and printouts.
2. Empowered Patients with the Super App
Calcium’s mobile Super App lets patients take control of their medication routine. They can:
- Log new medications or supplements
- Set reminders for doses and refills
- Track adherence and symptoms
- Share updates with their provider in real-time
This turns the patient into an active participant, rather than a passive subject.
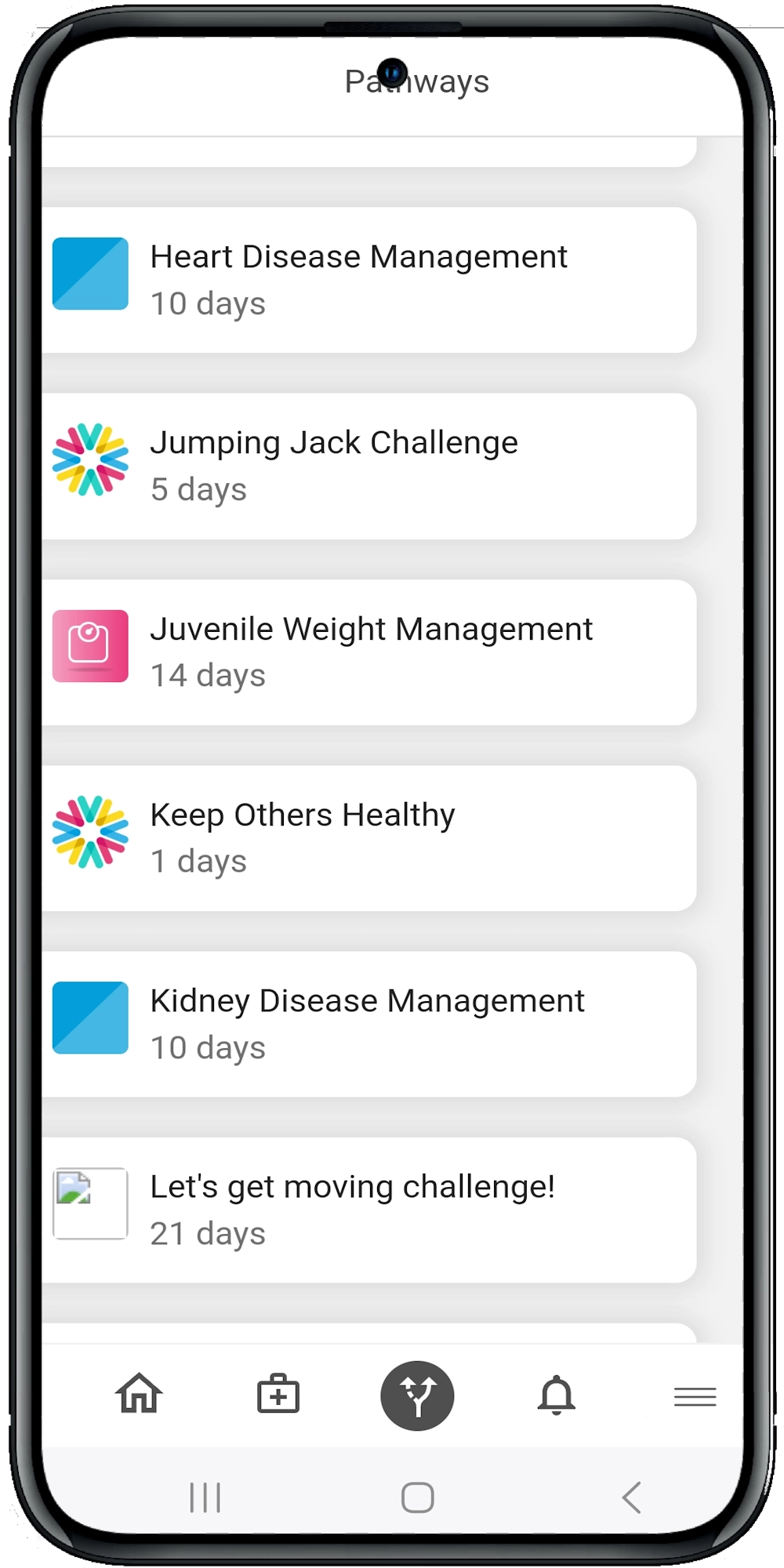
3. Smart Pathways with Embedded Medication Management
For chronic conditions or recovery periods, Calcium’s AI-powered health pathways include:
- Daily check-ins for medication adherence
- Side effect monitoring
- Pre- and post-procedure instructions that include med timing and safety tips
This isn’t just a record it’s a proactive care plan that helps patients stay on track.
4. Secure Sharing Without Friction
Patients can share their medication history with their doctors, caregivers or emergency responders instantly and securely. Whether it’s a routine visit or a crisis, the right people have the right info, at the right time.
And because the system is fully HIPAA-compliant, providers and patients alike can trust that sensitive medication data is protected.
Medication History as a Living Record, Not a Static List
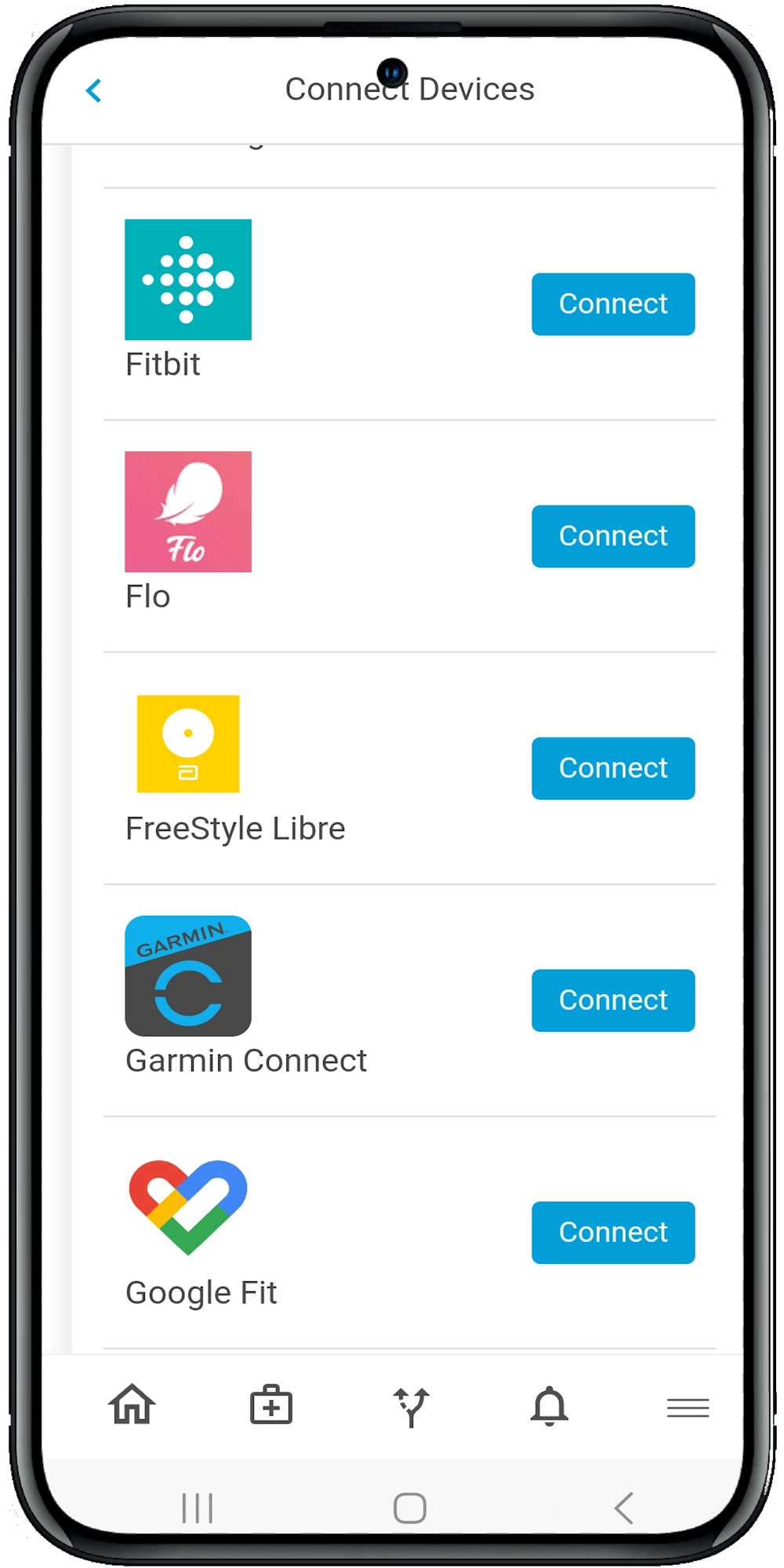
Traditional EHRs treat medication history like a snapshot a list updated once a year, if that. Calcium treats it like a living record that evolves alongside the patient’s health journey.
With integration into Apple Health, Fitbit, Dexcom and other connected devices, the Calcium platform doesn’t just record data it listens to it. That context can help flag changes in blood pressure, glucose, weight or heart rate that signal a medication isn’t working or needs adjustment.
It’s the difference between reading yesterday’s weather and checking a live radar map.
The Wrap
In the fast-moving world of healthcare, you can’t afford blind spots especially when it comes to your patients’ medications. Whether you’re treating chronic conditions, managing acute care or coordinating across multiple providers, access to complete, real-time medication history can change outcomes.
The old way of relying on memory, manual records or patchy EHRs no longer cuts it. With the Calcium digital health platform, you’re not just filling in the gaps you’re stepping into a smarter, safer way to deliver care. Our provider tools and patient-facing Super App work together to track, sync and share medication data effortlessly, empowering better decisions and better outcomes.
Reference
-
- Kalra D. (2006). Electronic health record standards. Yearbook of medical informatics, 136–144. https://pubmed.ncbi.nlm.nih.gov/17051307/
- Ambinder E. P. (2005). A history of the shift toward full computerization of medicine. Journal of oncology practice, 1(2), 54–56. https://doi.org/10.1200/JOP.2005.1.2.54
- Hoerbst, A., & Ammenwerth, E. (2010). Electronic health records. A systematic review on quality requirements. Methods of information in medicine, 49(4), 320–336. https://doi.org/10.3414/ME10-01-0038
- Häyrinen, K., Saranto, K., & Nykänen, P. (2008). Definition, structure, content, use and impacts of electronic health records: A review of the research literature. International Journal of Medical Informatics, 77(5), 291–304. Elsevier Ireland Ltd. Retrieved from https://doi.org/10.1016/j.ijmedinf.2007.09.001
- Safran, C., & Goldberg, H. (2000). Electronic patient records and the impact of the Internet. International Journal of Medical Informatics, 60(1), 77–83. https://doi.org/10.1016/S1386-5056(00)00106-4
- Hassey, A., Gerrett, D., & Wilson, A. (2001). A survey of validity and utility of electronic patient records in a general practice. BMJ, 322(7299), 1401–1405. https://doi.org/10.1136/bmj.322.7299.1401
- Greenhalgh, T., Potts, H. W. W., Wong, G., Bark, P., & Swinglehurst, D. (2009). Tensions and paradoxes in electronic patient record research: A systematic literature review using the meta-narrative method. The Milbank Quarterly, 87(4), 729–788. https://doi.org/10.1111/j.1468-0009.2009.00578.x