Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
What You Need to Know Before Investing in a Care Management Platform for Accountable Care Organizations
If you’re leading an Accountable Care Organization (ACO)—or thinking about joining one—you already know the pressure is real. Balancing cost control with high-quality care isn’t just a mission; it’s a mandate. And while software is supposed to make that easier, most so-called “ACO software” leaves organizations drowning in data but starving for insight.
The truth? Choosing the wrong platform can quietly sabotage your value-based care goals before you even get started.
The right ACO platform, on the other hand, can be a game-changer—fueling better patient outcomes, smoother operations, and measurable financial return. But with so many systems promising the moon, how do you separate hype from real impact? If you’ve ever wondered why your current tools aren’t moving the needle—or how to make a smarter investment—this post is for you. Let’s unpack what truly matters in ACO software and how to choose a solution that delivers what you actually need: real, sustainable ROI.
What Does ROI Really Mean for ACO Software?
When you’re evaluating ACO software, it’s tempting to think of ROI purely in dollar signs. But in today’s healthcare landscape, true return on investment stretches beyond the bottom line.
In reality, the ROI for a population health management tool should be multidimensional:
- Financial: Yes, you want to reduce the total cost of care, but it also means fewer hospitalizations, fewer readmissions, and lower medication waste.
- Clinical: You need better health outcomes—especially in chronic conditions like diabetes, heart disease, and mental health.
- Operational: ROI also means your care team spends less time chasing faxes and more time supporting patients.
- Behavioral: Don’t underestimate the power of engaging patients in their own care. Adherence, after all, is half the battle.
Recent studies have also explored ROI through the lens of employee wellness programs using ACO-based platforms. One 12-month evaluation showed measurable ROI when organizations integrated ACO software to track and enhance workplace health outcomes, reinforcing the broader applicability of these tools beyond traditional clinical settings (Hartung, 2016).
ACO performance isn’t just measured by how much money you save. It’s about how much value you deliver across the entire continuum of care. If your software can’t track or contribute to that value, it’s not delivering real ROI.
What Features Should ACO Software Include to Drive Real Results?
Not all ACO software is built the same. Some platforms were designed a decade ago, built for compliance and documentation—not for real-time, value-based care.
To choose a solution that actually works in the trenches, make sure it includes these seven core capabilities:
1. Data Integration That Actually Works
Goodbye, data silos. ACOs deal with fragmented data—EHRs, claims, pharmacies, labs, wearables—and the right software needs to pull all that together.
Look for:
- EHR and pharmacy system integration
- API connections to labs, health plans, and population health platforms
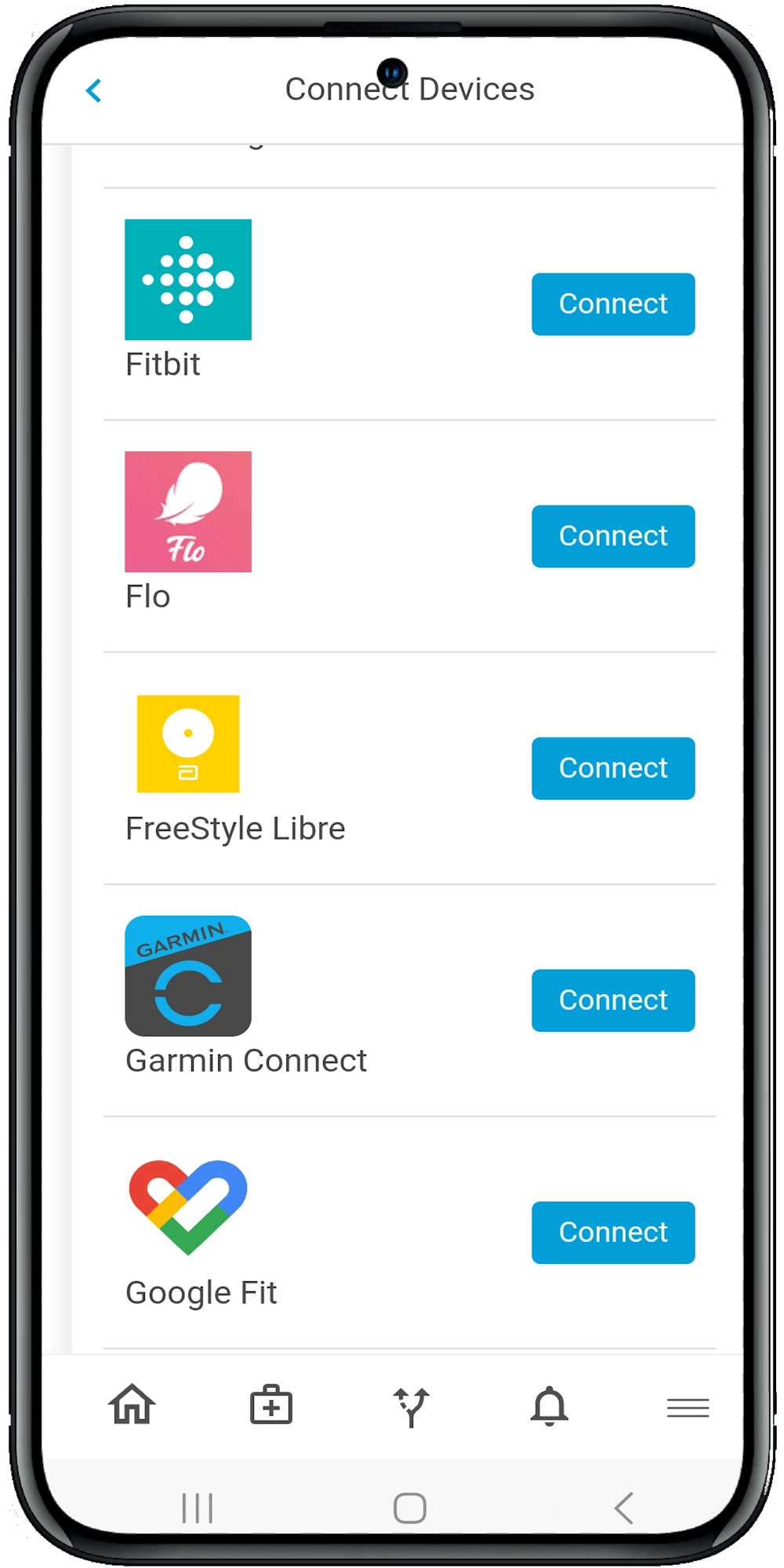
- Device and app syncing for real-time patient monitoring
The more complete the picture, the more precise your interventions will be.
2. Strong Care Management Tools
Can your care team quickly identify who’s at risk? Can they act on it immediately?
An effective digital health infrastructure includes:
- Real-time risk scoring
- Automated task assignments
- Smart alerts for missed check-ins or medication non-adherence
This helps prioritize the right patients at the right time—without drowning your team in dashboards.
3. Built-In Behavioral Health Features
Behavioral health isn’t optional. It’s a core component of whole-person care and a major cost driver in ACO populations.
Make sure the software supports:
- Depression and anxiety screening tools
- Behavioral health pathway integration
- Secure messaging with mental health providers
Integrated behavioral health tools help bridge the gap between physical and mental health—which is often where traditional ACOs fall short.
4. Medication Optimization Capabilities
Let’s be honest—medications are often where things go off the rails. Polypharmacy, non-adherence, poor reconciliation—it adds up fast.
According to a 2017 study, most ACOs struggle to manage the cost of medications, even though more than 70% of care visits involve prescriptions. Only 31% of ACOs felt well-prepared to manage med costs (Wilks et al., 2017).
So, what should your software do?
- Trigger alerts for duplications or interactions
- Track pharmacy fills and refills
- Suggest lower-cost therapeutic alternatives
- Support MTM and pharmacist workflows
If your software isn’t helping your pharmacists and care coordinators optimize medication use, it lacks a major opportunity to improve outcomes and control spending.
5. Engagement Tools That Patients Actually Use
You can’t expect results if patients aren’t showing up—digitally or physically.
Here’s what to look for in patient-facing tools:
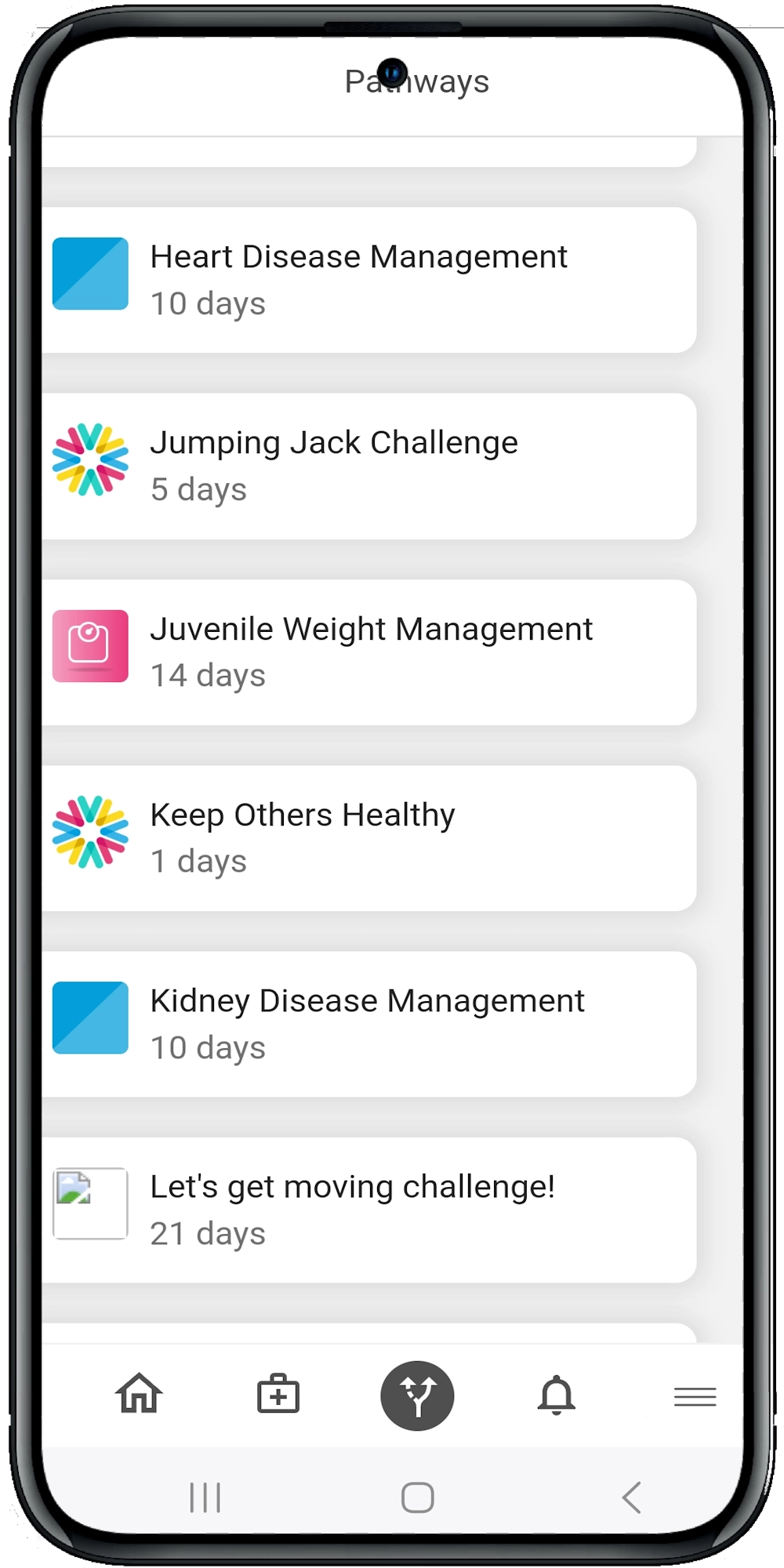
- Self-guided care pathways for chronic and preventive conditions
- Push notifications for meds, vitals, appointments, and exercise
- Symptom journaling and health goal tracking
- Motivational nudges and gamification features
The Calcium platform, for example, uses “digital pathways” that feel more like a personal coach than a clunky app. It adapts as users engage, sends timely prompts, and even helps patients understand their next step. That kind of real-time behavioral feedback loop is what keeps people engaged and improving.
6. Built-In ROI Tracking and Analytics
You can’t improve what you can’t measure. Your software should help you see what’s working—and what’s not.
Ask vendors:
- Does your platform calculate cost savings in real time?
- Can we filter ROI by condition, provider, or care plan?
- Do you track quality measure improvements tied to interventions?
A 2023 study on ACO care management in North Carolina showed a gradual but measurable reduction in per-member-per-month spending when care teams focused on long-term chronic disease management, SDOH, and behavioral health. But that took time—and software capable of tracking long-term impact (Rote et al., 2023).
Don’t rely on guesswork. ROI analytics should be clear, customizable, and built into your workflow.
7. SDOH Screening and Closed-Loop Referrals
If you’re not accounting for social determinants of health, you’re not treating the whole person.
Make sure your software supports:
- SDOH screening (housing, food, transportation, etc.)
- Integration with community-based organizations
- Referral tracking and confirmation (i.e., closed-loop)
This isn’t just a “nice-to-have.” Addressing SDOH can lead to major cost savings by reducing avoidable ER visits and hospitalizations. The Mission Health Partners ACO, for example, saw spending drop as patients engaged with social services alongside medical care (Rote et al., 2023).
Why Most ACO Software Fails to Deliver
Let’s face it: Many ACO platforms overpromise and underdeliver.
Here’s what often goes wrong:
- Disjointed data: Systems don’t talk to each other.
- Static care plans: One-size-fits-all pathways don’t engage real people.
- Minimal patient involvement: If the app’s not on their home screen, it’s not being used.
- No behavioral or mental health support: A gaping hole in care continuity.
- Weak analytics: No clear way to attribute results to actions.
A pilot program published in Circulation found that joining a Medicare ACO didn’t significantly reduce the use of discretionary cardiovascular imaging or procedures. The likely reason? Lack of patient engagement and insufficient decision support to influence care patterns (Colla et al., 2014).
What Does Good ACO Software Actually Look Like?
Think of ACO software as your organization’s GPS for population health. You need it to reroute in real time, avoid dead ends, and get you to your destination with minimal detours.
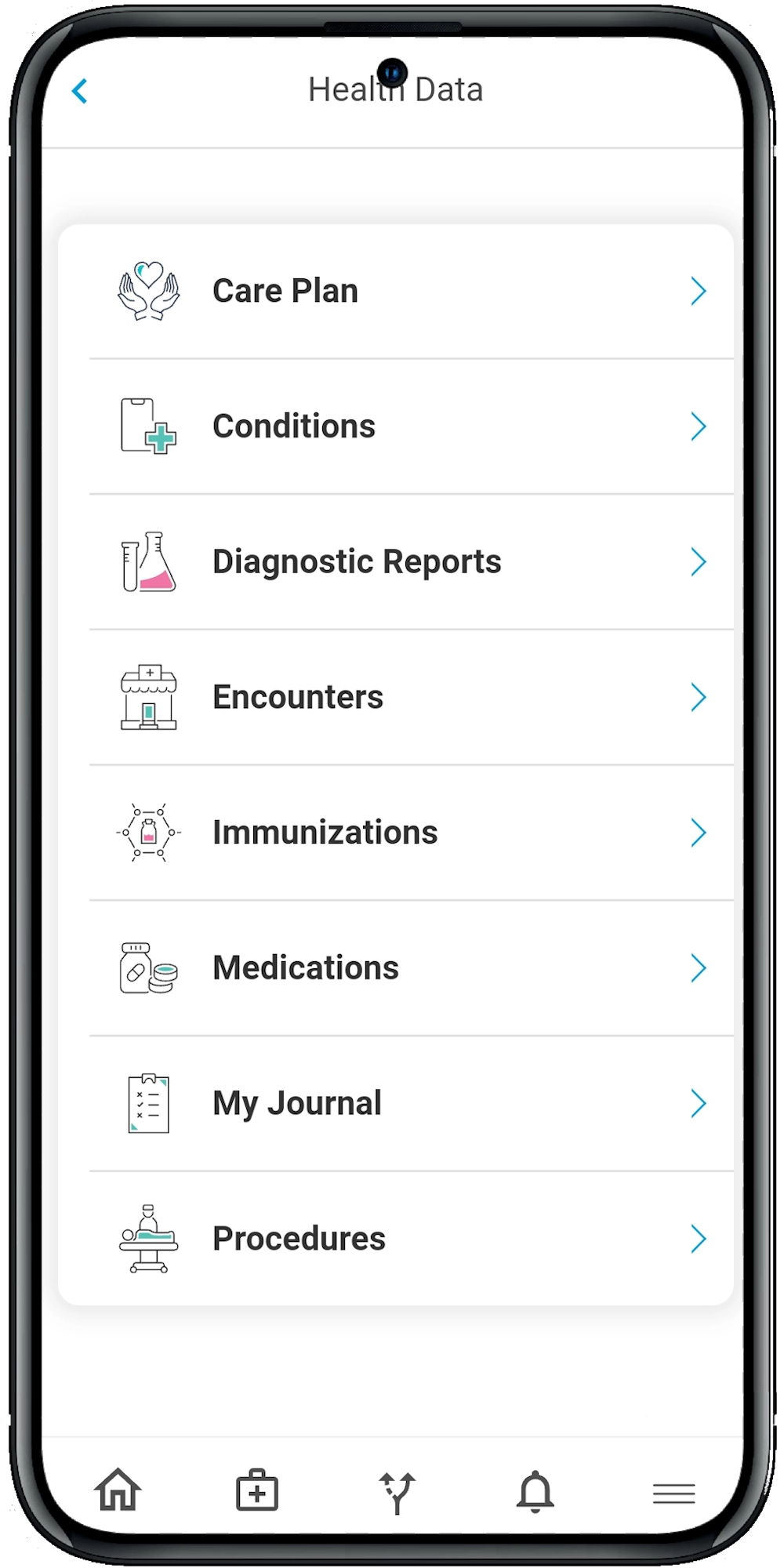
A solution like Calcium’s Digital Health Platform hits the mark by combining:
- A care team dashboard (Calcium Core)
- A patient-facing app with adaptive digital pathways
- Real-time health data integration
- AI-powered personalization
- Secure sharing across patients, providers, and family caregivers
It’s not about fancy features—it’s about driving real behavior change, tracking outcomes, and optimizing every dollar you spend.
The Wrap
Choosing ACO software isn’t just an IT decision—it’s a strategic move that can shape your organization’s clinical outcomes, patient experience, and financial future.
The stakes are too high to settle for tools that simply check regulatory boxes. You need a platform that helps your team work smarter, connects patients to meaningful support, and delivers measurable return on investment. If you’re ready to move beyond spreadsheets and static dashboards, it’s time to explore a more dynamic, patient-centered solution.
The Calcium digital health platform was built for organizations like yours—those ready to lead in value-based care, behavioral health, and whole-person engagement. From real-time data insights to personalized digital care pathways, Calcium offers the tools and flexibility ACOs need to thrive. Want to see how it works in action? Visit Calcium Health to learn more, schedule a demo, or start a conversation with our team. Let’s build better outcomes—together.
Reference
Hartung, A. J. (2016). Measuring Return-on-Investment (ROI) of a Worksite Wellness Program Using an Accountable Care Organization Software Program: What is the ROI at 12 Months? MEDICA. https://medica-musc.researchcommons.org/theses/429/
Wilks, C., Krisle, E., Westrich, K., Lunner, K., Muhlestein, D., & Dubois, R. (2017). Optimization of Medication Use at Accountable Care Organizations. Journal of Managed Care & Specialty Pharmacy, 23(10), 1054–1064. https://doi.org/10.18553/jmcp.2017.23.10.1054
Rote, E., Perloff, J., Lanou, A., Bartholomew, K., & Russell, A. (2023). Exploring Patient Spending in an ACO-Sponsored Care Management Program: A Case Study. (2023). The American Journal of Accountable Care, 11(3), 5–12. https://doi.org/10.37765/ajac.2023.89433
Colla, C. H., Goodney, P. P., Lewis, V. A., Nallamothu, B. K., Gottlieb, D. J., & Meara, E. (2014). Implementation of a Pilot Accountable Care Organization Payment Model and the Use of Discretionary and Nondiscretionary Cardiovascular Care. Circulation, 130(22), 1954–1961. https://doi.org/10.1161/circulationaha.114.011470