Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
Closing the Gap Between Appointments with Smarter, Connected Care
We’re now in a fast-moving, data-driven world, but healthcare still struggles with a surprisingly old problem: knowing what’s really going on with a patient right now. Providers are expected to make critical decisions with incomplete data, while patients are often left navigating their health alone between appointments. And despite the billions spent on electronic health records and digital tools, most systems still don’t talk to each other.
That disconnect isn’t just frustrating — it’s dangerous.
What if there were a better way? A way to pull together all the fragmented pieces of health data — from hospital visits to home devices — and turn it into a real-time, actionable view of patient health?
The Current Digital Health Data Landscape
Digital health data is everywhere — tucked inside EHR systems, streaming from your Fitbit, stored in your phone’s wellness apps, even living inside lab portals. But while data is abundant, it’s rarely connected. That’s the paradox. We’re rich in information but poor in insights.
However, most of today’s healthcare systems are still stuck in a fragmented ecosystem. Hospitals use one platform, clinics use another, and your wearable device? That’s not even part of the conversation in many care settings.
Then there’s the issue with traditional electronic health records. If EHRs were meant to be the nervous system of healthcare, they’re acting more like file cabinets. Decades of research — like Kalra’s study on interoperability — show that EHRs often fail to “speak the same language,” making it nearly impossible to transfer meaningful health data between systems.
And when physicians do manage to get the data, it’s often stripped of context. Imagine trying to finish a puzzle with half the pieces missing — that’s what providers face when they rely solely on traditional EHRs. Another study by Ambinder paints the picture clearly: even in high-stakes fields like oncology, EHRs often make care delivery harder, not easier.
Add to that clunky interfaces, inconsistent data quality, and a general lack of patient involvement, and it’s no wonder clinicians feel like they’re wrestling with outdated software instead of using tools that help them heal.
What Real-Time Patient Monitoring Actually Requires
For real-time patient monitoring to be more than just a buzzword, healthcare systems need to get three things right. Without these pillars, any digital health strategy is just a house of cards.
1. Unified, Interoperable Infrastructure
First, everything has to work together — EHRs, apps, wearables, and devices. If your patient is tracking their blood pressure at home or using Apple Health to monitor their steps, that data should flow directly to the provider’s dashboard in real time.
This is where many platforms fall short. Without true interoperability (built on standards like HL7 and FHIR), you’re left with a digital Tower of Babel — everyone’s talking, but no one understands each other.
2. Security Without Sacrificing Access
It’s one thing to collect health data. It’s another to protect it. A modern system has to balance bulletproof security (think HIPAA compliance, audit logs, role-based access) with the flexibility for patients to share data with caregivers, providers or even family members — all on their own terms.
3. A Patient-Centric Experience
Let’s face it: if patients don’t use the tools, the tools are useless. That means intuitive design, clear feedback, and features that help patients take control of their health journey — like reminders, motivational nudges and easy data sharing. Because if your app feels like homework, no one’s going to do it.
How Calcium Powers Real-Time Monitoring From Every Angle
This is where the Calcium digital health platform flips the script. Instead of trying to patch up broken systems, Calcium takes a fresh approach — one that connects the dots between patients, data and care teams in real time.
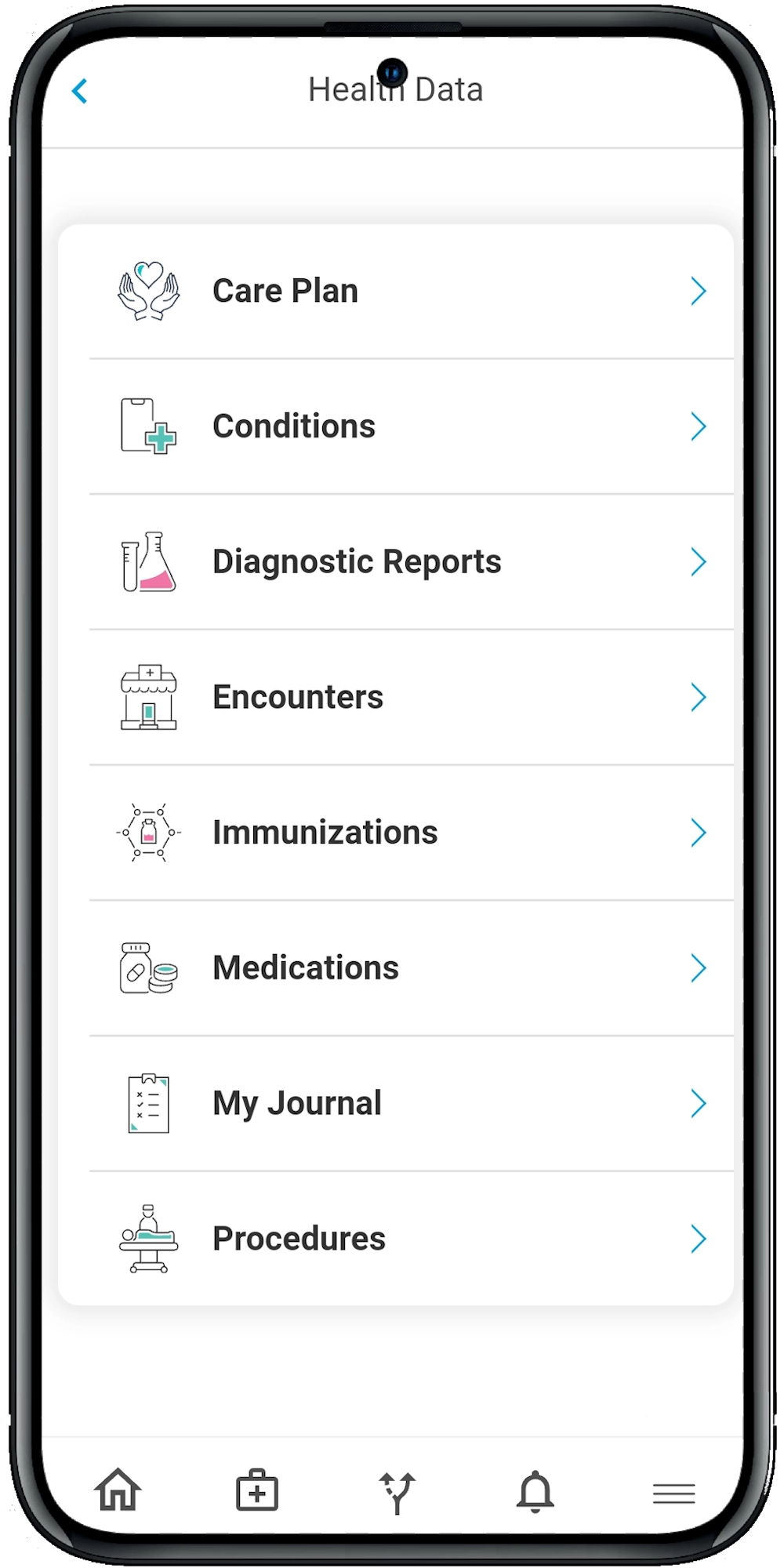
The Calcium Super App: Built for People, Not Portals
The Calcium Super App is like a personal health coach that fits in your pocket. Patients can track everything from vitals and medications to journal entries and symptoms. But what really makes it powerful is integration.
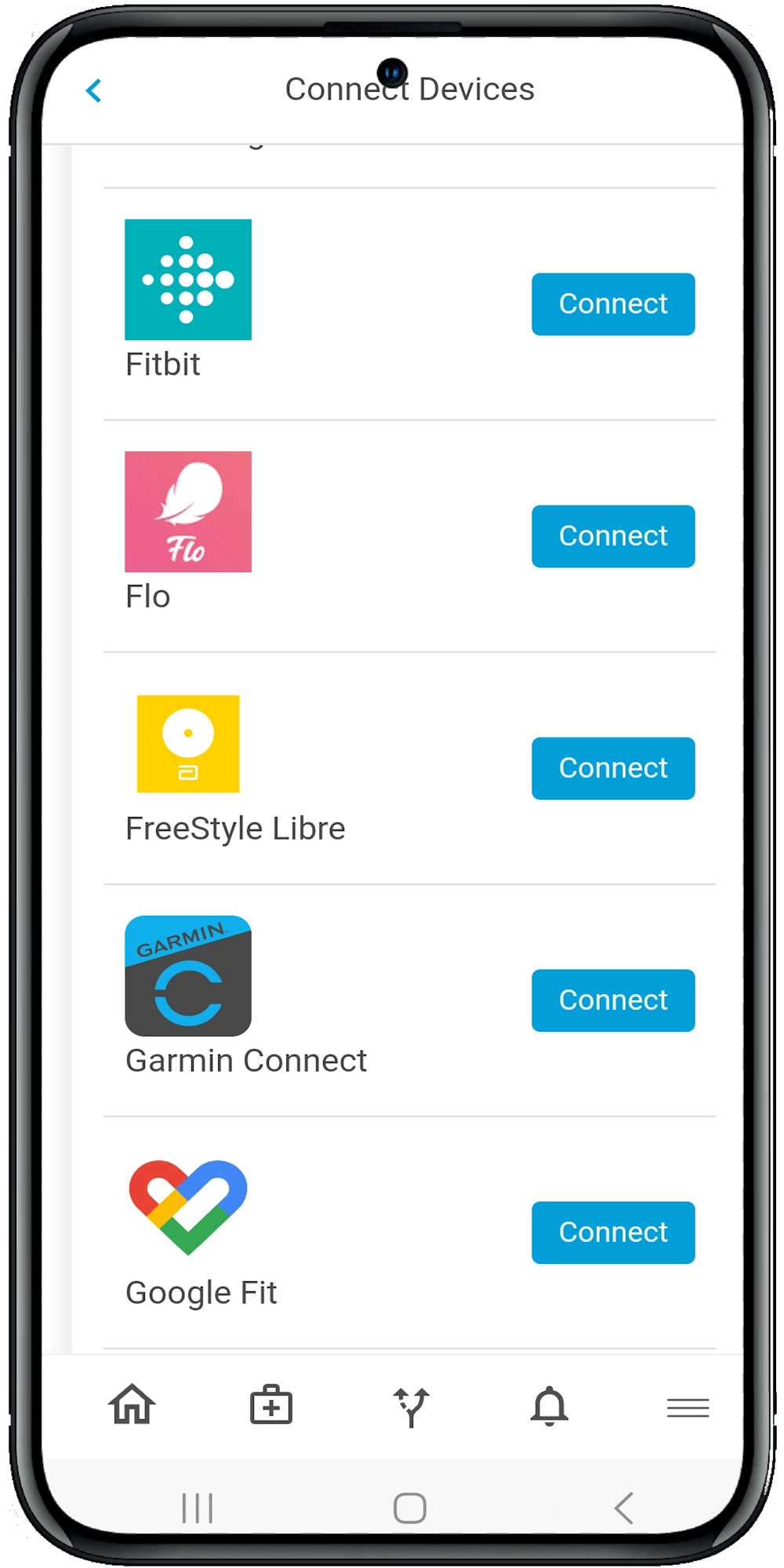
The app connects with a huge range of devices and platforms — Apple Health, Google Fit, Dexcom, Omron, Fitbit, Withings — so all your health data streams into one clean, digestible view. No more toggling between apps. No more trying to remember which device tracks what.
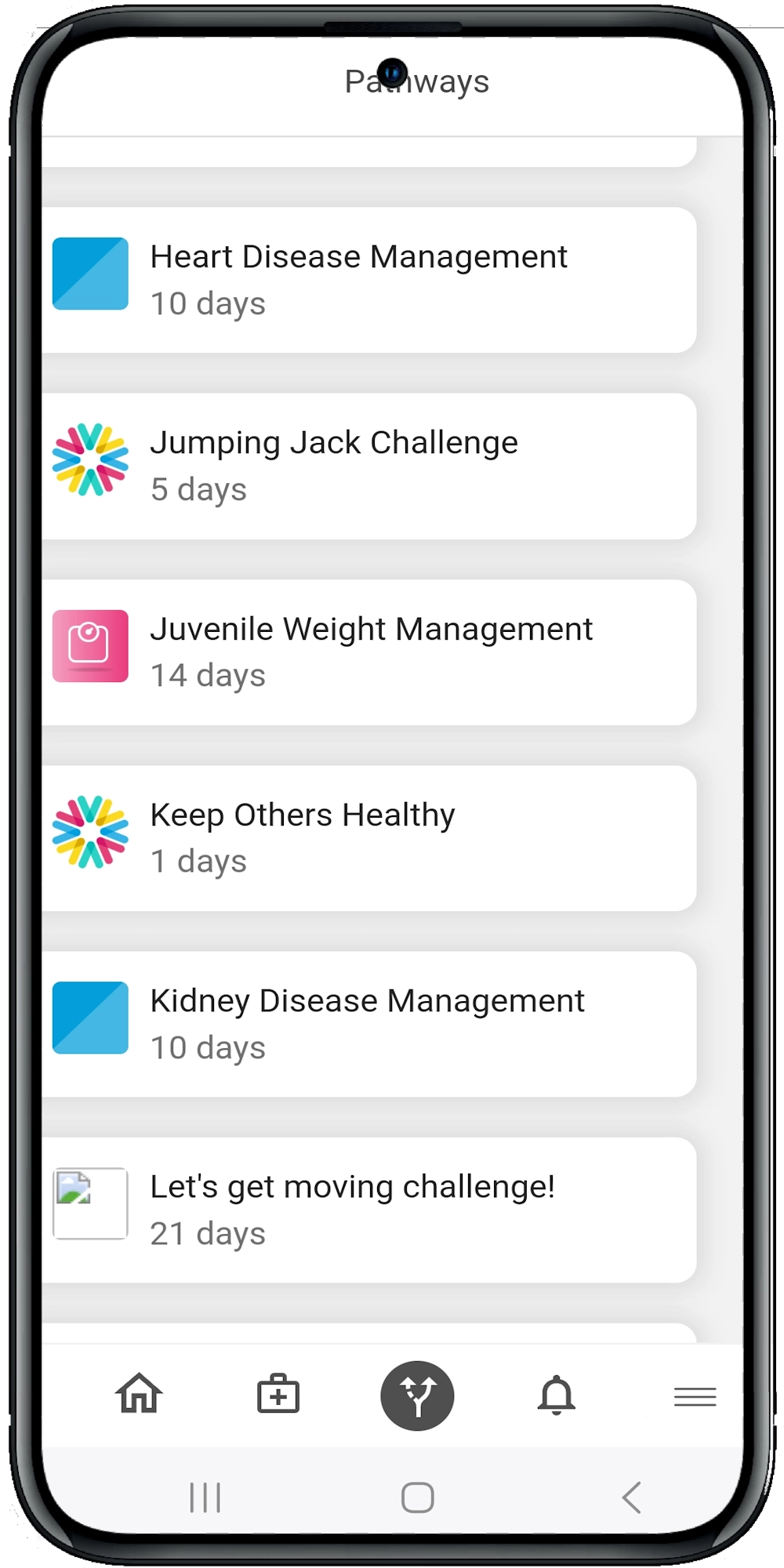
And here’s the kicker: patients can enroll in digital pathways that offer daily guidance for managing chronic conditions, recovering from surgery or improving general wellness. These pathways aren’t just generic checklists — they’re personalized, interactive, and powered by real data.
Calcium Core: The Provider’s Command Center
On the clinician side, Calcium Core acts as the control tower. It gives care teams real-time access to patient vitals, alerts, medication logs, and pathway progress — all in one HIPAA-compliant dashboard.
So, let’s say your patient with hypertension stops logging their blood pressure or skips a pathway step. Calcium alerts the provider before that patient becomes a readmission risk. It’s proactive care instead of reactive scrambling.
Providers can also assign pathways, track outcomes, and generate population health insights. Whether you’re managing 10 patients or 10,000, the data is always organized, actionable and updated live.
Real-Life Use Cases: Where Calcium Shines
So what does this look like in the real world? Here are a few ways providers and patients are using Calcium today:
Chronic Condition Monitoring
Let’s say a patient with Type 2 diabetes is using a continuous glucose monitor at home. The data feeds directly into the Super App, then into the provider’s Core dashboard. If glucose levels spike outside the norm, both patient and provider are alerted — allowing for timely adjustments before things spiral.
Post-Surgical Recovery
After a hip replacement, patients can follow a guided pathway with daily mobility exercises, medication reminders, and symptom tracking. Providers get real-time progress updates and can intervene early if complications arise. It’s like remote physical therapy and case management, all rolled into one.
Preventive & Behavioral Health
Whether it’s managing anxiety, quitting smoking or increasing daily steps, Calcium’s motivational pathways and reminders keep users engaged. Pathways gamify health with progress bars, achievements and educational nudges — because health goals feel more doable when they’re broken into bite-sized tasks.
Measuring What Matters: Aligning with Value-Based Care
All this data isn’t just for show. Calcium helps providers hit the key metrics that drive value-based reimbursement:
- Improved outcomes (fewer readmissions, better chronic disease control)
- Higher patient satisfaction (through transparency, ease of use, and empowerment)
- Greater efficiency (by reducing manual follow-ups and unnecessary visits)
In fact, as highlighted in one of the uploaded research articles, real-time EPR systems — when designed correctly — not only boost accuracy but also reduce cognitive burden on clinicians. Calcium builds on that idea by turning raw data into smart, structured insights that help both sides of the care equation.
The Wrap
Real-time patient monitoring isn’t just a nice-to-have — it’s the future of effective, patient-centered care. But to get there, we need tools that go beyond the status quo. Platforms like Calcium don’t just collect digital health data; they make it work for patients and providers — in real time, at scale, and with a level of personalization that legacy systems simply can’t match.
Whether you’re a healthcare leader looking to improve outcomes, or a provider who wants to stay connected to patients between visits, Calcium offers the tools to bridge the gap. From unified data dashboards to AI-powered care pathways, it’s all about turning insight into action — and action into better health.
Reference
- Kalra, D. (2006). Electronic Health Record Standards. In R. Haux & C. Kulikowski (Eds.), IMIA Yearbook of Medical Informatics 2006 (pp. 136–144). IMIA and Schattauer GmbH. Retrieved from https://www.schattauer.de (Accessed April 9, 2025).
- Ambinder, E. P. (2005). Oncology Enters the Information Age. Journal of Oncology Practice, 1(2), 57–63. Retrieved from https://www.jopasco.org (Accessed April 9, 2025).
- Hoerbst, A., & Ammenwerth, E. (2010). Electronic Health Records: A Systematic Review on Quality Requirements. Methods of Information in Medicine, 49(4), 1–9. Schattauer GmbH. Retrieved from https://www.schattauer.de (Accessed April 9, 2025).
- Häyrinen, K., Saranto, K., & Nykänen, P. (2008). Definition, structure, content, use and impacts of electronic health records: A review of the research literature. International Journal of Medical Informatics, 77(5), 291–304. Elsevier Ireland Ltd. Retrieved from https://doi.org/10.1016/j.ijmedinf.2007.09.001 (Accessed April 9, 2025).
- Safran, C., & Goldberg, H. (2000). Electronic patient records and the impact of the Internet. International Journal of Medical Informatics, 60(1), 77–83. https://doi.org/10.1016/S1386-5056(00)00106-4
- Hassey, A., Gerrett, D., & Wilson, A. (2001). A survey of validity and utility of electronic patient records in a general practice. BMJ, 322(7299), 1401–1405. https://doi.org/10.1136/bmj.322.7299.1401
- Greenhalgh, T., Potts, H. W. W., Wong, G., Bark, P., & Swinglehurst, D. (2009). Tensions and paradoxes in electronic patient record research: A systematic literature review using the meta-narrative method. The Milbank Quarterly, 87(4), 729–788. https://doi.org/10.1111/j.1468-0009.2009.00578.x