Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
Breaking Down Barriers Between Systems, People and the Personalized Care They Deserve
Have you ever wondered why your doctor’s office doesn’t seem to know what happened at your last specialist visit — or why you still have to carry around paperwork in the age of smartphones?
The truth is, our healthcare system is rich in data but poor in connection. Information lives in silos, bouncing between clinics, hospitals, pharmacies and devices without ever truly syncing. That disconnect doesn’t just create frustration — it affects outcomes, slows care and leaves patients and providers operating in the dark.
As healthcare shifts toward personalization and prevention, the ability to access and act on complete, real-time health data has never been more critical. So why is true interoperability still so elusive, and what would it take to finally make it a reality? The answers might surprise you — and the solution may already be within reach.
What Is Health Data Interoperability — and Why Does It Matter?
Let’s start with the basics. Health data interoperability means that different healthcare systems — from hospitals to pharmacies to wearables — can communicate, exchange, and make sense of data in a meaningful way. It’s not just about sending files from Point A to Point B. It’s about sharing information that’s useful, timely, and accurate, so providers can actually act on it.
Think of it like speaking the same language. If one provider records blood pressure in one system, and another provider uses different units or a different format, the data may be lost in translation — or completely ignored. Without standardized formats, shared terminology, and real-time integration, the potential of health IT falls apart.
That’s the gap true interoperability fills. And it’s not just a tech upgrade — it’s the difference between reactive, siloed care and proactive, patient-centered decision-making.
The Seven Real-World Challenges Blocking Interoperability
Despite years of investment, most healthcare systems still struggle to connect the dots. Let’s break down the most common obstacles standing in the way of truly connected health.
1. Inconsistent Data Standards and Terminologies
One provider might code a condition using ICD-10, while another uses SNOMED. Lab results might follow different formatting rules. This inconsistency leads to disjointed records and errors in clinical interpretation.
Kalra’s research nails this point: without semantic interoperability — the ability to preserve clinical meaning when data moves between systems — records become static archives instead of living, useful resources.
2. Vendor Lock-In and Proprietary Platforms
Some EHR vendors design their systems to be closed-off, making it hard (or expensive) to integrate with other tools. This creates data silos and reinforces competition instead of collaboration.
That’s like a hospital using a phone that only works with its own brand — helpful internally, but useless in a healthcare ecosystem that demands teamwork.
3. Delayed or Non-Real-Time Data Exchange
In many cases, data is exchanged in batches or after-the-fact uploads. Providers are left working with outdated information, which defeats the purpose of having an electronic record in the first place.
If a patient’s blood pressure spikes at home and no one sees it until their next appointment, what’s the point? That lag can cost lives in high-risk populations.
4. Privacy and Consent Complexities
HIPAA compliance is essential, but it can also slow innovation. Questions around data ownership, patient consent, and sharing permissions often leave providers afraid to fully engage in data exchange.
Interoperability can’t thrive without clear, secure systems that honor privacy while giving patients control over how their data is shared and with whom.
5. Fragmentation Across the Continuum of Care
Hospitals. Primary care. Behavioral health. Urgent care. Rehab. Each uses different systems. And even within a single health system, departments may not be fully integrated.
This fragmentation means patients fall through the cracks. Discharge instructions may not make it to primary care, mental health providers may not know about recent surgeries, and duplicate tests pile up.
6. Lack of Integration with Consumer Health Tools
Wearables, fitness apps, blood glucose monitors — they all generate data that could be vital for preventive care. But most EHRs can’t integrate it.
Patients are generating valuable health insights daily, but without a way to bridge the gap between consumer tech and clinical systems, that data stays locked away.
7. Poor Usability in Clinical Workflows
Even when interoperability technically exists, the user experience is often terrible. Data might be there — buried in an obscure tab, buried in a PDF, or presented in a confusing format.
Ambinder’s research on oncology workflows showed how bad design can sabotage care. EHRs should support — not interrupt — clinical decision-making.
Why Interoperability Is the Key to Smarter, Personalized Care
Now let’s shift gears. When interoperability does work, the benefits aren’t just technical — they’re transformational.
Here’s what’s possible when data flows freely:
Real-Time Care Coordination
When providers can instantly see updates from a patient’s other clinicians, remote devices, or self-tracking tools, they can act faster. This means earlier interventions, fewer errors, and improved outcomes — especially in high-risk or chronic care populations.
Safer Medication Management
Interoperable systems help reconcile medication lists, detect potential drug interactions, and confirm that prescriptions are filled. No more guessing if a patient is taking something a specialist prescribed three months ago.
Seamless Transitions Between Providers
Hospital discharges, referrals to specialists, follow-ups — all run smoother when everyone has access to the same, updated patient record. Patients don’t have to retell their story at every visit.
Tailored Treatment Plans
When data from labs, devices, and daily routines are unified, providers can create care plans based on real trends — not just annual checkups. This kind of personalization is what turns episodic care into continuous, patient-driven health.
Empowered Patients
When patients can view, manage, and share their own health data, they become more engaged in their care. That leads to better compliance, stronger communication, and greater trust.
What the Research Says: EHRs Haven’t Delivered
Despite being the backbone of modern healthcare, traditional EHRs haven’t delivered on interoperability. The studies from Kalra, Ambinder, and Hoerbst & Ammenwerth all point to the same truth: EHRs lack interoperability, usability, and patient-centricity.
Hoerbst & Ammenwerth’s sweeping review found that most systems fail at the basics — secure access, seamless exchange, and intuitive use. They’re built for documentation, not action. And that’s exactly where smarter platforms must take the lead.
How the Calcium Digital Health Platform Bridges the Gap
The Calcium platform was designed from the ground up to solve what EHRs can’t — and to complete the health data picture for both patients and providers.
Here’s how it works:
1. Seamless Connectivity Across 95% of Health Systems
Calcium uses HL7 and FHIR protocols to pull data from hospitals, labs, pharmacies, and clinics — consolidating it into a single, unified record that’s patient-owned and provider-ready.
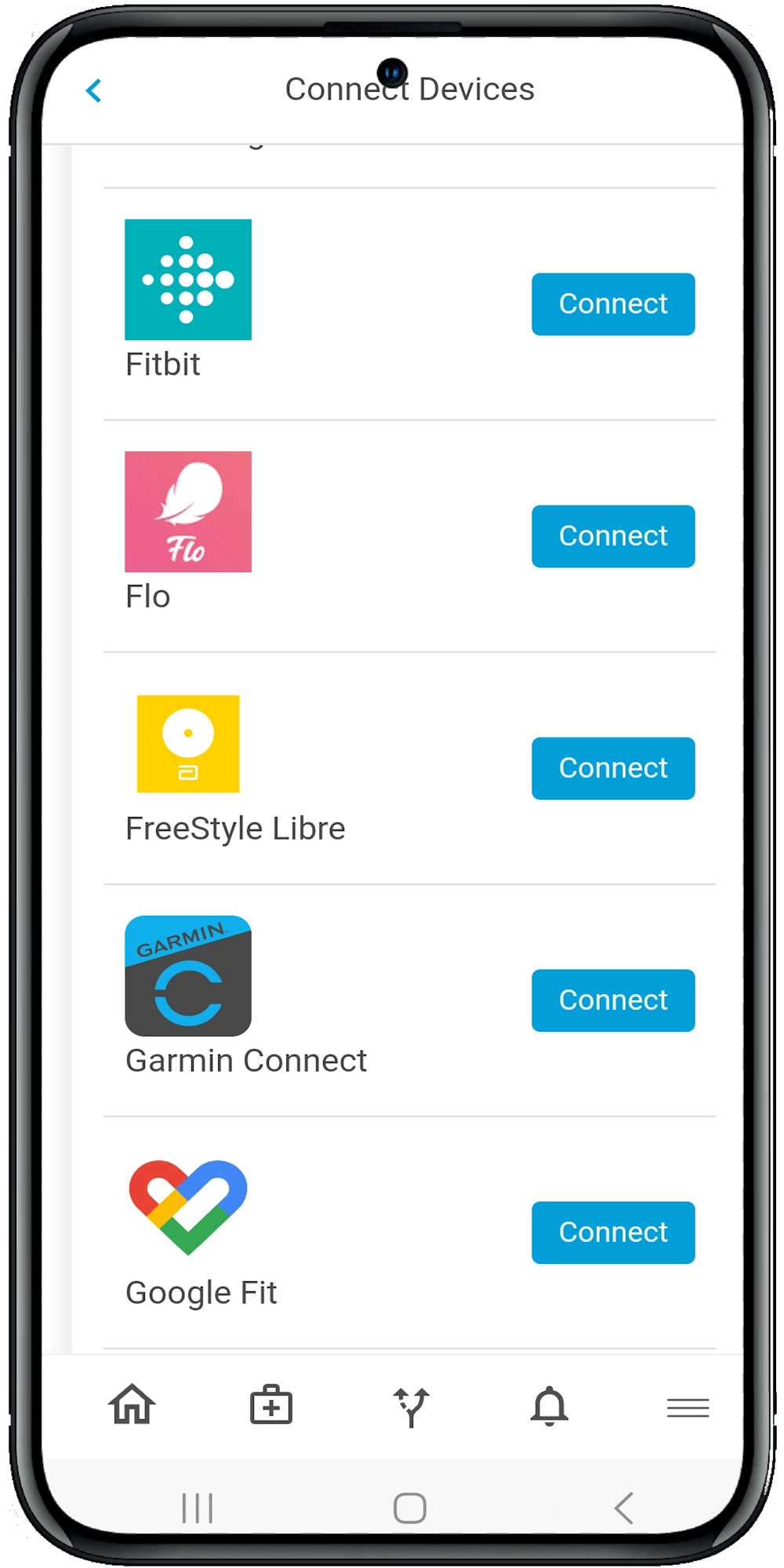
2. Real-Time Syncing with Devices and Apps
Through the Calcium Super App, patients can link Apple Health, Fitbit, glucose monitors, and more. Data flows instantly to the provider dashboard (Calcium Core), where clinicians can monitor trends in real-time.
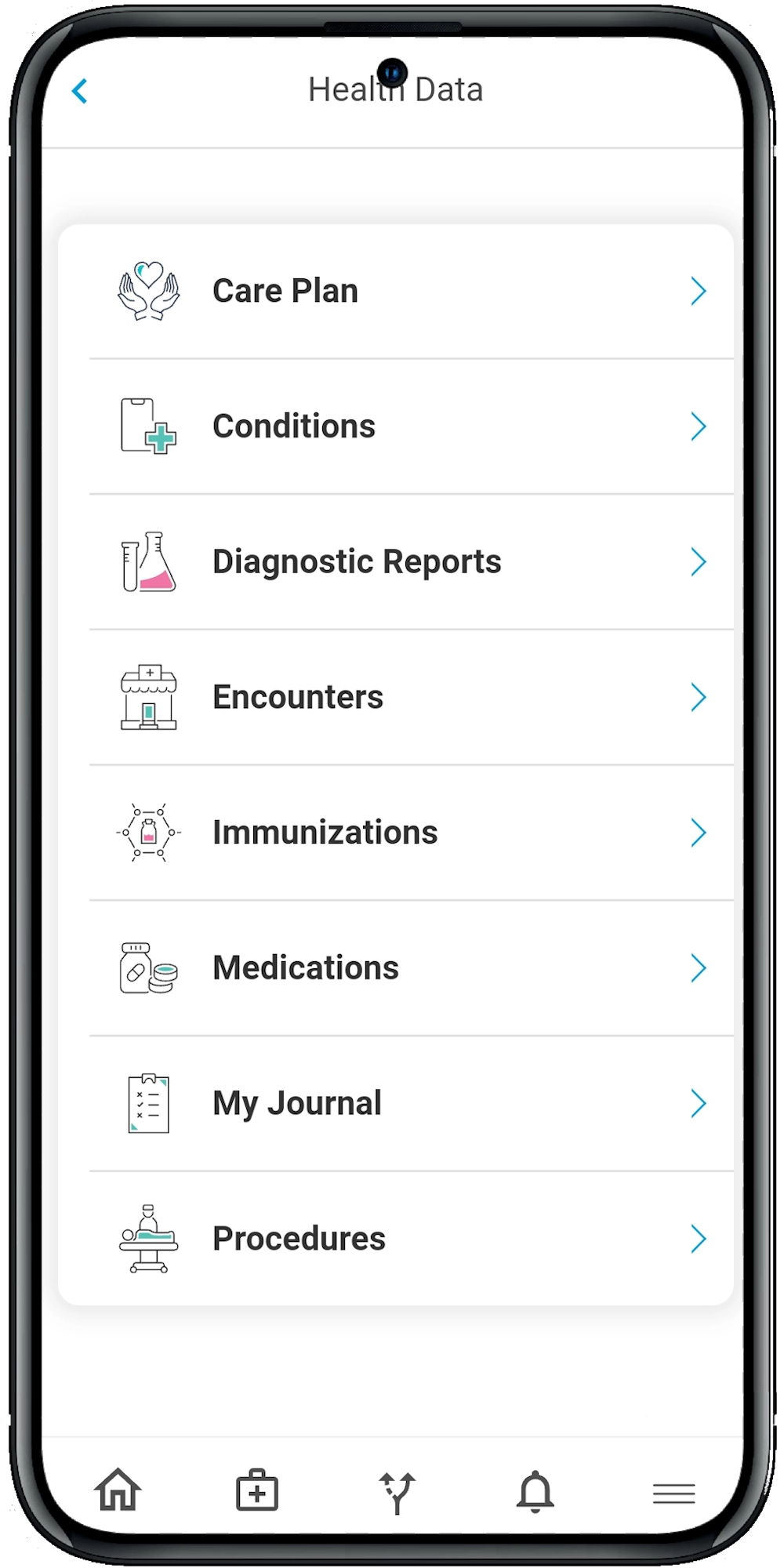
3. User-Friendly, Clinically Relevant Dashboards
Calcium Core was built for speed and clarity. Providers can filter by alerts, review care plans, track pathway progress, and access shared notes — all in a few clicks.
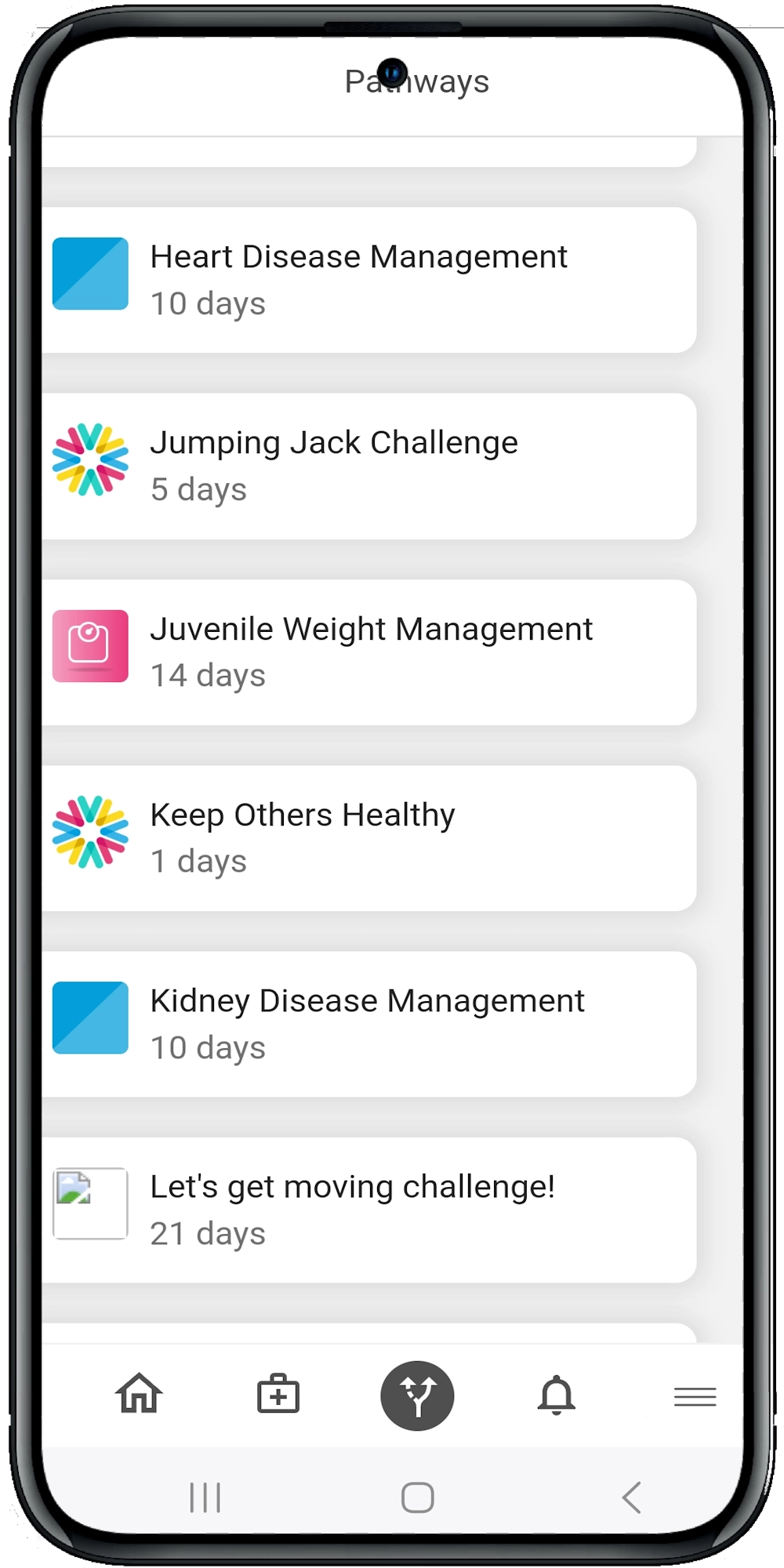
4. AI-Powered Personalized Pathways
Using real-time health data, providers can assign care pathways that adjust based on vitals, adherence, and patient feedback — from diabetes management to surgical recovery.
5. Secure, Transparent Data Sharing
Patients stay in control of their health data. They decide who gets access, how much they can see, and when it’s shared. Built-in audit trails and role-based access ensure full HIPAA compliance.
The Future: From Disconnected Records to Connected Care
Interoperability isn’t just a buzzword — it’s the foundation for personalized, proactive, and human-centered care. When systems speak the same language, everyone benefits: providers, patients, caregivers, and communities.
Health data interoperability isn’t a distant ideal — it’s the key to making care more human, more proactive and more precise. It means fewer blind spots, smarter decisions and stronger relationships between patients and providers.
But getting there requires more than just technical fixes. It calls for a platform that understands the real-world complexities of healthcare — from data fragmentation to workflow challenges to patient empowerment. That’s exactly what Calcium was built to solve. With seamless integration, real-time insights and intuitive tools for both providers and patients, the Calcium digital health platform turns disconnected records into meaningful, actionable health journeys.
Reference
- Kalra, D. (2006). Electronic Health Record Standards. In R. Haux & C. Kulikowski (Eds.), IMIA Yearbook of Medical Informatics 2006 (pp. 136–144). IMIA and Schattauer GmbH. Retrieved from https://www.schattauer.de.
- Ambinder, E. P. (2005). Oncology Enters the Information Age. Journal of Oncology Practice, 1(2), 57–63. Retrieved from https://www.jopasco.org.
- Hoerbst, A., & Ammenwerth, E. (2010). Electronic Health Records: A Systematic Review on Quality Requirements. Methods of Information in Medicine, 49(4), 1–9. Schattauer GmbH. Retrieved from https://www.schattauer.de.
- Häyrinen, K., Saranto, K., & Nykänen, P. (2008). Definition, structure, content, use and impacts of electronic health records: A review of the research literature. International Journal of Medical Informatics, 77(5), 291–304. Elsevier Ireland Ltd. Retrieved from https://doi.org/10.1016/j.ijmedinf.2007.09.001