Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
Unlocking the full potential of health data to improve care, reduce errors and empower patients.
In healthcare, timing isn’t just everything—it can be the difference between a quick recovery and a missed diagnosis. Yet too often, delays happen not because of a lack of skill or urgency, but because the right information isn’t available when it’s needed most.
Picture this: a specialist sits down to review a patient’s case, only to discover key lab results are trapped in another provider’s system. Or a patient gets a new prescription that unknowingly conflicts with a medication from another doctor.
Unfortunately, these aren’t rare scenarios—they’re daily obstacles caused by fragmented digital health records. As we move deeper into value-based care, it’s clear: we don’t just need more data—we need better, smarter, more connected records. So how can we fix what’s broken? And how do we ensure digital patient records actually help, instead of hinder, modern care? Let’s explore the future of healthcare data done right.
Why Digital Patient Records Still Leave So Much to Be Desired
For all the investment poured into electronic health records (EHRs), most healthcare professionals would agree—they’re still not delivering what was promised. Instead of seamless access and smarter care, providers often wrestle with clunky systems, siloed data and missing context. It’s not just frustrating. It’s dangerous.
Studies show that when records are incomplete or slow to surface, patients pay the price. Diagnoses get delayed. Medications get duplicated. And providers are left guessing without the full story in front of them. Kalra’s research in 2006 made it clear: without true interoperability and shared clinical meaning, digital records become digital paperweights—technically available but practically unusable.
What’s Holding Digital Patient Records Back?
Let’s take a closer look at why digital records haven’t lived up to the hype. Each of these issues can create real risk for patients and real headaches for providers.
Here are the top 7 challenges standing in the way:
1. Siloed Systems
Most EHRs don’t talk to each other. A patient might have records spread across a dozen systems—none of which connect. You end up with a digital jigsaw puzzle that never quite fits together.
2. Fragmented Health Histories
Even if data is available, it’s often incomplete. A primary care doctor might not see a recent ER visit. A surgeon might not know about the patient’s current medication list. That disconnect can slow care down or send it in the wrong direction.
3. Poor User Experience
Ambinder’s study on oncology practices showed just how hard it is to use EHRs in real clinical workflows. When digital tools feel like a burden, not a benefit, providers disengage—and patient care suffers.
4. Outdated or Delayed Data
Many EHRs only reflect what happens inside clinic walls. But today’s patients generate health data 24/7—through wearables, smart devices and home tests. If your record system can’t keep up in real time, it’s already behind.
5. Weak Security Controls
Some systems still lack basic protections like two-factor authentication or user-specific access levels. That leaves data vulnerable—not only to breaches but also to misuse within the system.
6. Limited Patient Access
Despite regulations that mandate patient access to records, many portals remain hard to navigate, incomplete or locked behind red tape. If patients can’t see or share their own health info, how can they truly participate in their care?
7. Missing Clinical Context
A pile of labs, notes and medications isn’t enough. Providers need the why behind each test, diagnosis and prescription. Without it, they’re left piecing together intent from breadcrumbs.
Faster Diagnoses Start With Smarter Records
Now let’s talk solutions—because digital patient records can be powerful when they’re designed right.
When providers have full, real-time access to a patient’s health history, they can make decisions faster and with more confidence. Imagine the time saved when a new specialist can review your latest labs, scan your recent imaging and see your chronic conditions—all before the first appointment.
Here’s how better records accelerate the diagnostic process:
- Fewer delays between visits – No more waiting on faxes or phone calls.
- Reduced need for repeat testing – Providers can see what’s already been done.
- Improved triage and prioritization – Risk factors are visible early.
- Better collaboration between teams – Everyone works from the same data set.
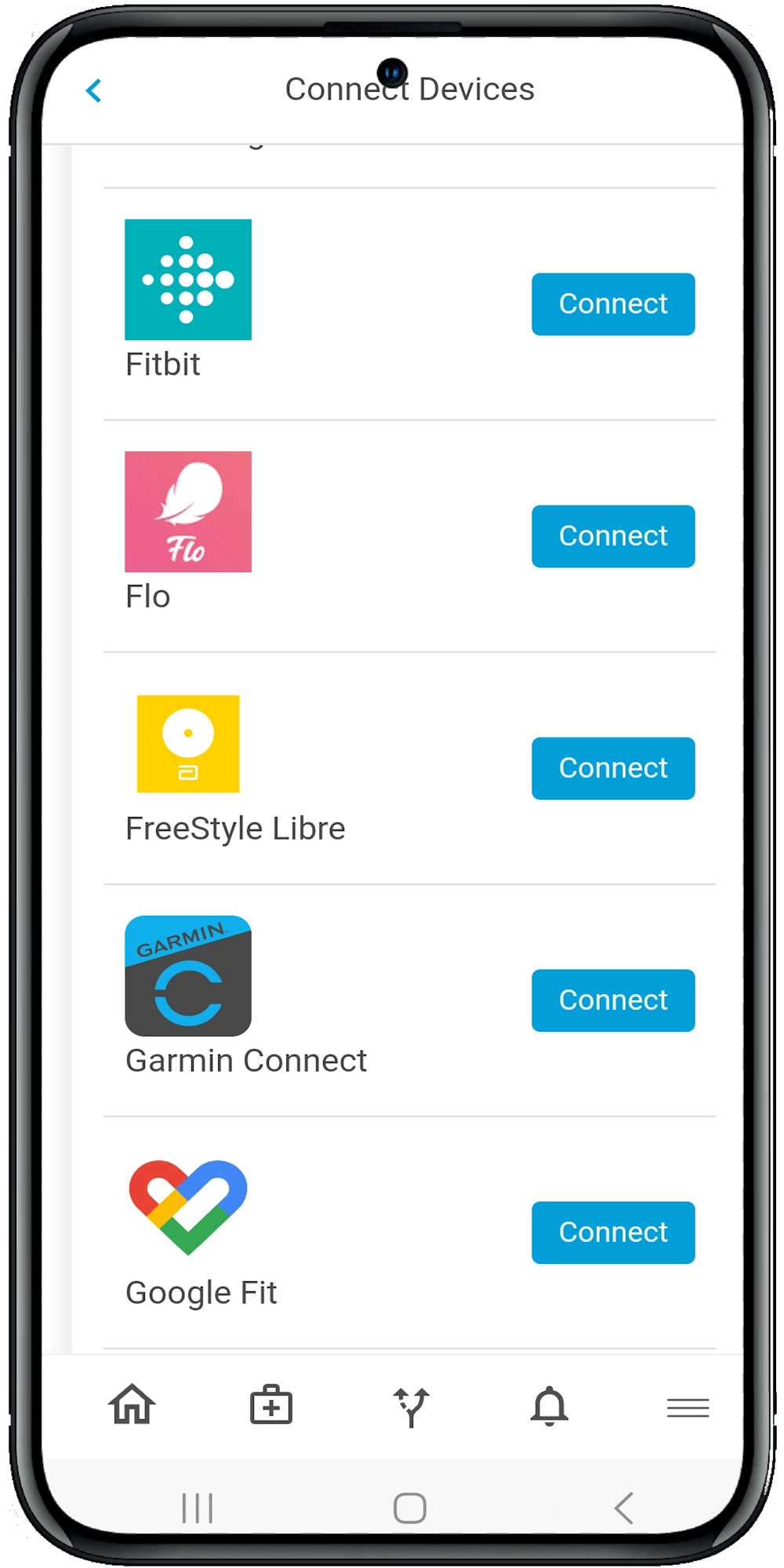
Calcium’s platform was built for this. With integration into over 95% of U.S. health systems using HL7 and FHIR standards, Calcium pulls in labs, diagnoses, notes and more—into one patient-controlled record. Even better, it integrates real-time vitals from devices like Apple Watch, Dexcom and Omron.
Safer Prescribing Starts With the Full Story
Let’s be honest—prescribing mistakes isn’t always about negligence. Sometimes they happen because the provider simply didn’t know. Maybe a patient forgot to mention another med. Maybe the pharmacy record didn’t sync. Maybe the EHR didn’t flag a dangerous interaction.
Safer prescribing requires visibility across systems, across visits and across time. That’s where digital records can be life-saving—literally.
Here’s what providers can do with smarter prescribing tools:
- Avoid drug interactions by seeing the full medication list.
- Catch duplicate prescriptions across different specialists.
- Check real-time vitals to adjust dosages appropriately.
- Monitor compliance through app-connected reminders and self-reporting.
- Share medication info securely with caregivers and family.
Calcium’s Super App includes a built-in Medication Manager, where users can track prescriptions, supplements and reminders. Providers, using the Calcium Core dashboard, can view this in real time, along with alerts that flag potential issues. It’s safer for patients—and simpler for clinicians.
Why Patient Empowerment Makes All the Difference
Let’s flip the script. What happens when patients have full access to their digital records?
They become active partners in care. They can prepare questions before visits, spot inconsistencies, and even detect when something looks off. More importantly, they can share their data with whomever they trust—be it a specialist, a second opinion provider, or a family caregiver.
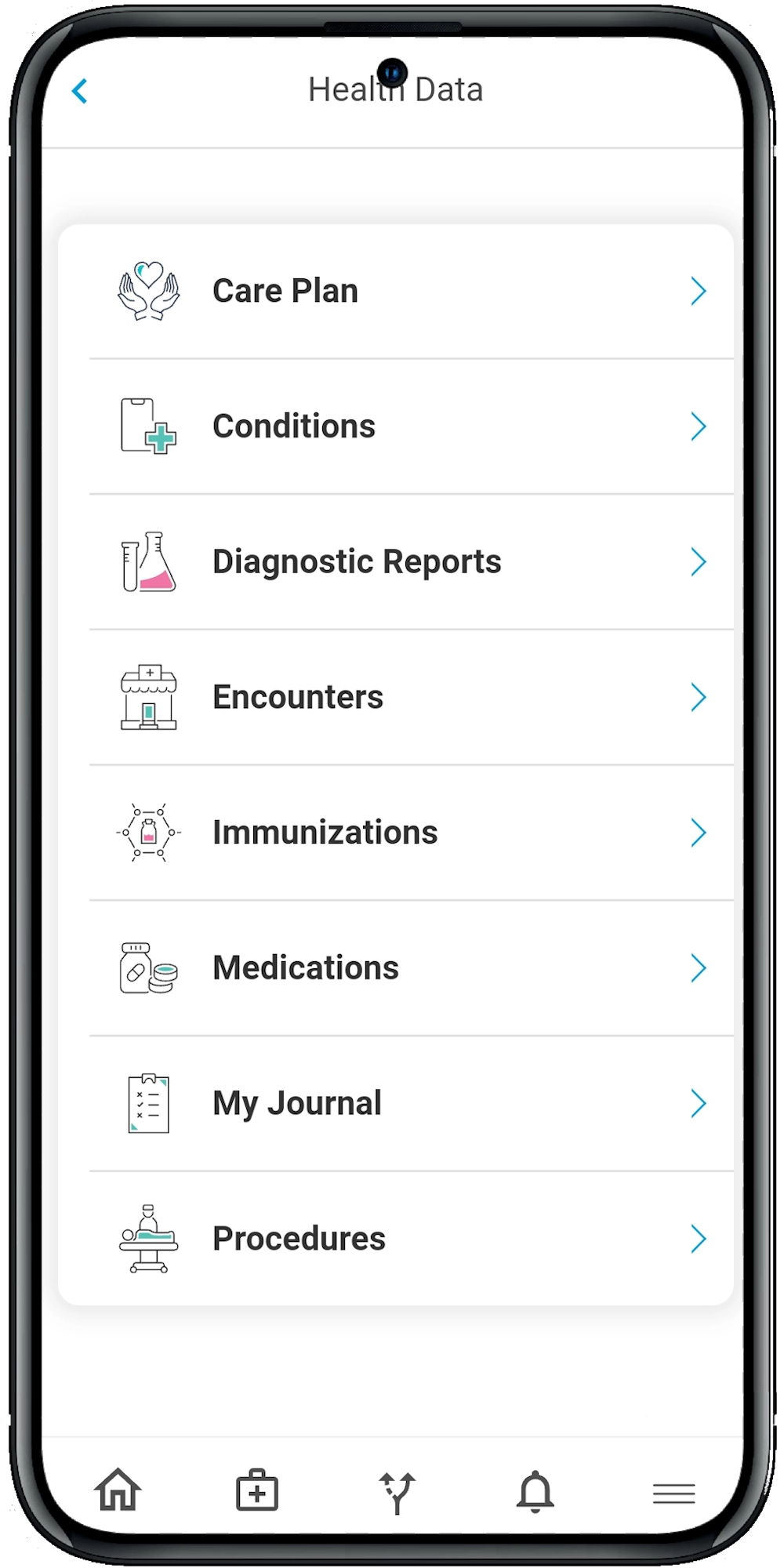
In the Calcium ecosystem, patients don’t just read their records. They:
- Track and log their symptoms
- Sync wearable and device data
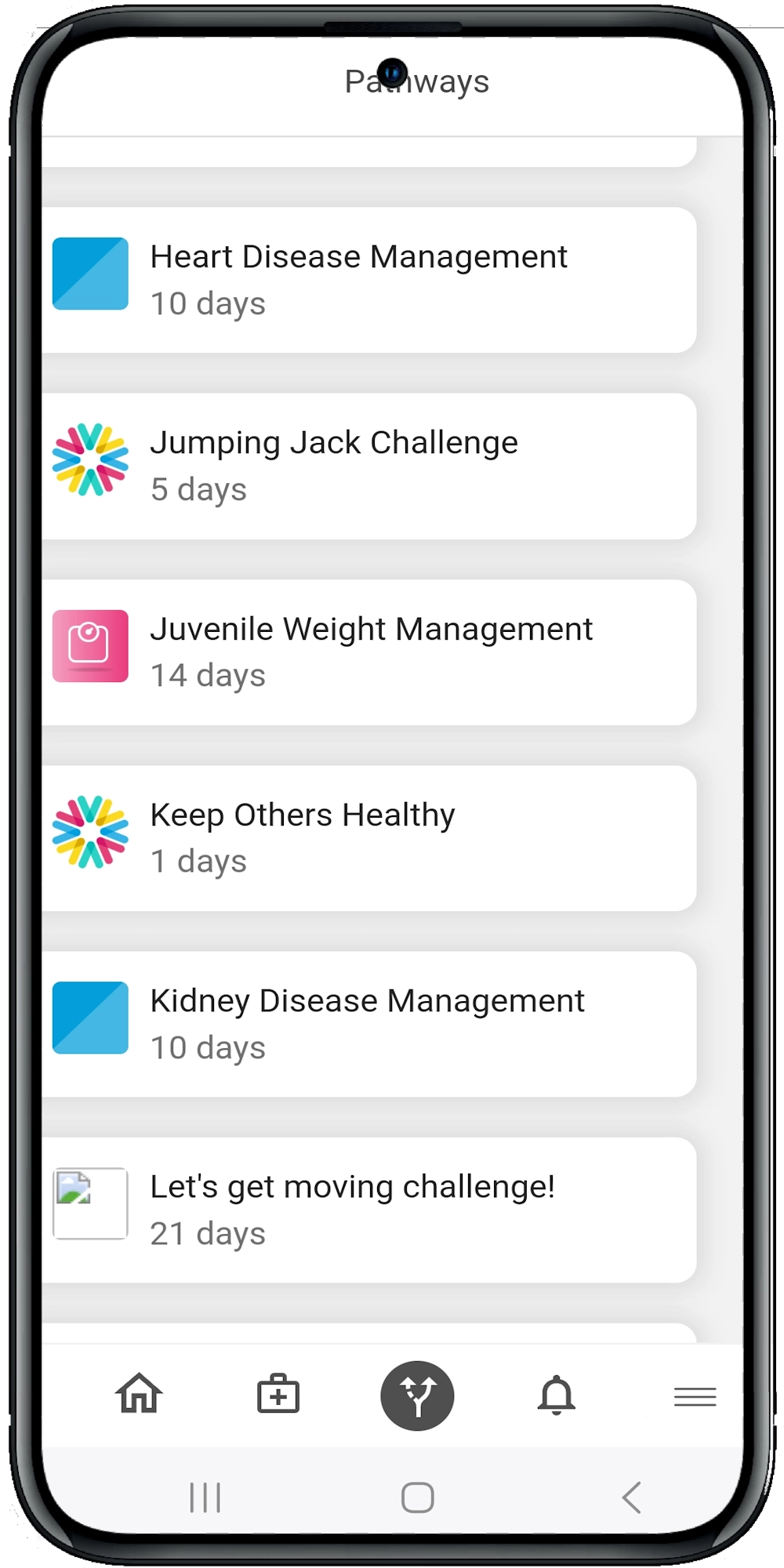
- Follow guided care pathways
- Journal health experiences in real time
- Share access with providers and loved ones
It’s the kind of empowerment that boosts adherence, lowers anxiety and improves long-term outcomes. And in the world of value-based care, that kind of patient engagement is a win for everyone.
Why Health Systems Should Prioritize Record Transformation
As care moves toward value-based models, outcomes matter more than volume. And outcomes are driven by information—how fast it flows, how complete it is and how well it’s used.
That’s why improving digital patient records isn’t just a tech upgrade. It’s a strategic shift.
Healthcare organizations that invest in smarter records can expect:
- Reduced readmissions
- Improved medication adherence
- Faster diagnoses and treatment starts
- Lower administrative costs
- Higher patient satisfaction scores
The key is not to replace existing EHRs—but to enhance them. Calcium does just that. It complements traditional systems by adding real-time data, patient tools and a unified record that spans across providers, devices and health events.
With AI-powered care pathways, HIPAA-compliant sharing tools and a mobile-first interface, Calcium turns digital records into actionable health intelligence.
The Wrap
It’s no longer enough for digital records to simply exist—they have to work for us.
When patient data flows securely and intelligently across platforms, the result is better care, safer prescribing, and quicker answers for those who need them. That’s the power of truly connected health records.
The Calcium digital health platform is built to bridge the gaps legacy systems leave behind—bringing real-time data, smarter integration and patient-driven access to the forefront of care. Whether you’re a healthcare provider looking to streamline decision-making, or a patient ready to take control of your health journey, Calcium offers the tools to make it happen.
Reference
- Kalra D. (2006). Electronic health record standards. Yearbook of medical informatics, 136–144. https://pubmed.ncbi.nlm.nih.gov/17051307/
- Ambinder E. P. (2005). A history of the shift toward full computerization of medicine. Journal of oncology practice, 1(2), 54–56. https://doi.org/10.1200/JOP.2005.1.2.54
- Hoerbst, A., & Ammenwerth, E. (2010). Electronic health records. A systematic review on quality requirements. Methods of information in medicine, 49(4), 320–336. https://doi.org/10.3414/ME10-01-0038
- Häyrinen, K., Saranto, K., & Nykänen, P. (2008). Definition, structure, content, use and impacts of electronic health records: A review of the research literature. International Journal of Medical Informatics, 77(5), 291–304. Elsevier Ireland Ltd. Retrieved from https://doi.org/10.1016/j.ijmedinf.2007.09.001