Türkiye’de bahis severler için en çok tercih edilen bettilt giriş adreslerden biri olmaya devam ediyor.
Curacao lisanslı platformlar arasında güvenilirlik açısından üst sıralarda bahsegel giriş yer alan, uluslararası denetimlerden başarıyla geçmiştir.
Kazançlı bahis deneyimi arayan herkes için bettilt doğru seçimdir.
Rulet masalarında en çok tercih edilen bahis türleri arasında kırmızı/siyah ve tek/çift seçenekleri yer alır; pinco giriş bu türleri destekler.
Basketbol tutkunları için en iyi kupon fırsatları bettilt sayfasında yer alıyor.
A Smarter Way to Guide Patients Home and Keep Them on Track
Surgical recovery doesn’t end when the patient leaves the operating room—it’s only just beginning. For Ambulatory Surgery Centers (ASCs), where speed, efficiency, and patient turnover are everything, post-op recovery can feel like a black box. Patients go home, and providers hope for the best.
But in today’s value-based care environment, hope isn’t a strategy. ASCs are being judged not just on what happens inside their walls, but on what happens days and weeks later. Complications, readmissions, and patient satisfaction now directly impact revenue and reputation.
The solution? A well-designed digital recovery plan.
Yet most ASCs are still operating with outdated tools—or none at all. That’s a missed opportunity. A smart, connected recovery strategy isn’t just a nice-to-have; it’s a must-have for ASCs that want to lead in a competitive, outcomes-driven market. So, how can ASCs reimagine recovery in the digital age? Let’s dig into that next.
The Evolution of ASCs in a Value-Based Era
ASCs are no longer just convenient alternatives to hospitals; they’re now front-runners in reshaping outpatient surgical care.
Over 5,300 ASCs now perform more than 23 million procedures annually in the U.S. alone. As the demand for same-day, low-acuity procedures grows, so does the pressure on ASCs to deliver safer recoveries, better outcomes, and higher patient satisfaction.
Here’s the catch: value-based care isn’t just about what happens in the operating room. It’s about what happens after. Recovery is where the rubber meets the road for metrics like readmission rates, follow-up compliance, and quality-adjusted life years (QALYs). Without a digital recovery plan, many ASCs risk falling behind on these critical indicators.
The 7 Biggest Challenges of Digital Post-Op Recovery for ASCs
So why aren’t more ASCs embracing digital recovery plans? Let’s unpack the top seven obstacles getting in the way.
1. Low Use of Health IT and EHRs
You’d expect most ASCs to have integrated electronic health records by now, right? Not quite. In one study, 47% of ASCs reported no use of EHRs, while over one-third lacked even basic digital functionality. That’s like trying to run a marathon in flip-flops.
2. Poor Communication During Care Transitions
Patient hand-offs are where things get messy. Important details—like medication schedules or red flags—can slip through the cracks. Without digital continuity, these transitions are high-risk events that can lead to complications, delayed recovery, or unnecessary emergency room visits.
3. Lack of Interoperability
Even when an ASC uses digital tools, it often doesn’t talk to each other. One platform handles pre-operative instructions, another tracks follow-ups, and neither integrates with the patient’s primary care physician (PCP) or specialist. This data fragmentation is a major barrier to seamless care coordination.
4. Inconsistent Enhanced Recovery Protocols (ERAS)
Enhanced Recovery After Surgery (ERAS) programs are designed to streamline recovery, reduce opioid use, and get patients moving faster. But in ASCs, ERAS implementation varies widely and often lacks digital tracking. Without consistent application and feedback loops, their benefits are watered down.
5. No Real-Time Post-Op Monitoring
Imagine trying to drive across the country with no dashboard. That’s what recovery looks like for most ASCs. Once patients go home, providers are flying blind. Without tools to monitor pain levels, medication adherence, or signs of infection, problems are often caught too late.
6. Weak Patient Engagement
Patients want convenience. But if a recovery app is clunky or hard to use, they’ll delete it faster than you can say “HIPAA.” Many ASCs don’t offer personalised digital tools that keep patients engaged and motivated post-surgery.
7. Reimbursement and Regulatory Hurdles
Let’s not ignore the elephant in the room—payment. Telehealth and digital recovery services have come a long way since COVID-19, but inconsistent reimbursement policies and a lack of billing codes still hold ASCs back.
What Should a Digital Recovery Plan Include?
Now that we’ve covered the roadblocks, let’s look at what an ideal digital recovery plan for ASCs should include. If you’re building from scratch, here are five core elements to focus on.
1. Preoperative Digital Prep
Think of this as the “training camp” before surgery. A solid recovery starts with strong preparation. ASCs should offer:
- Interactive video modules to explain what to expect
- Digital checklists for medications, fasting, and logistics
- Screening tools for anxiety, depression, or social risk factors
- Virtual consent forms and reminders
These tools don’t just reduce no-shows. They also help patients feel more confident and calm going into surgery, a key factor in recovery.
2. Seamless Data Integration
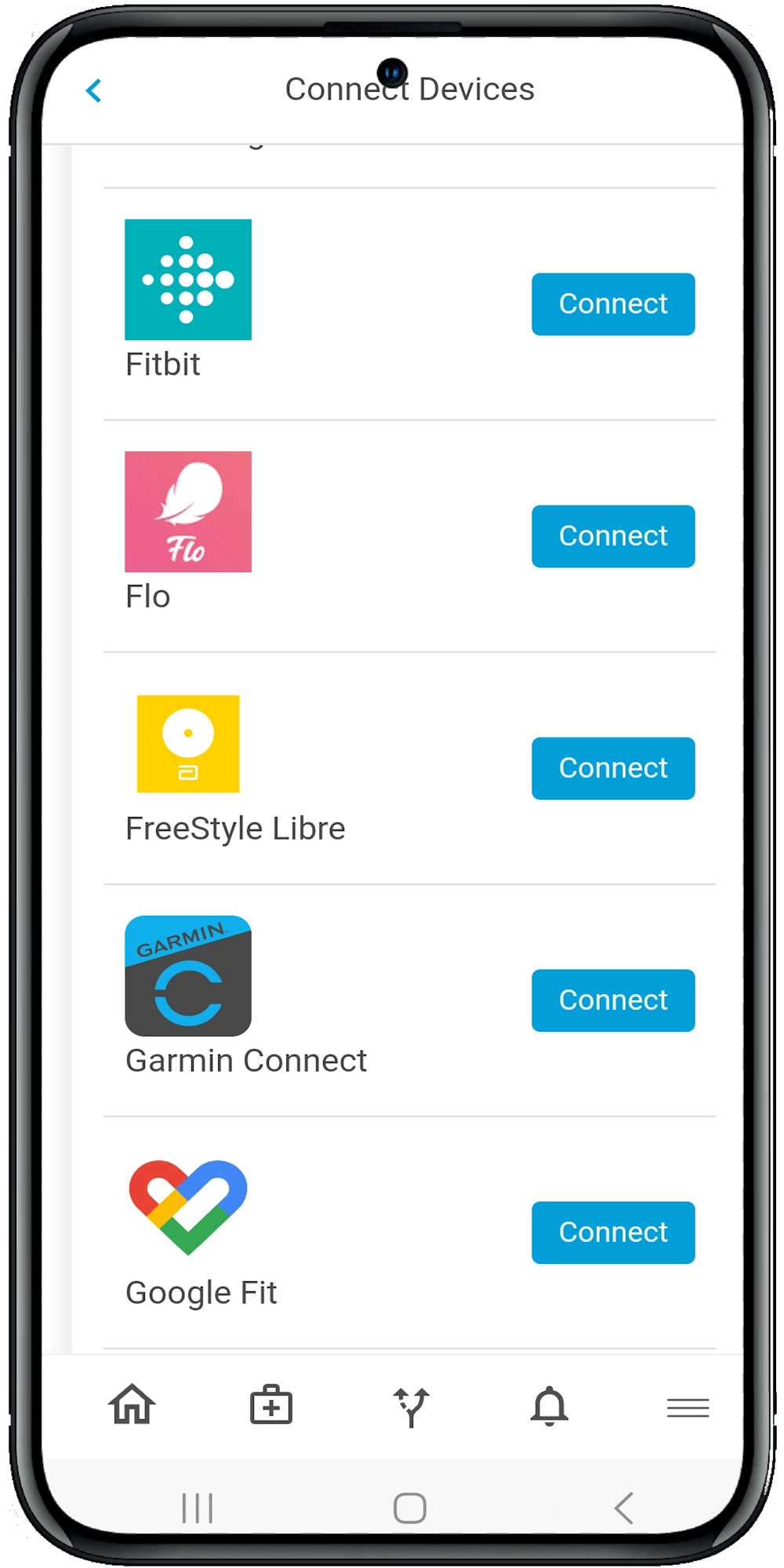
Patients shouldn’t have to repeat their health history five times. Digital recovery plans must plug into EHRs, scheduling systems, and even wearables when possible. Interoperability is the foundation for real-time updates, quality tracking, and smooth transitions across providers.
3. Real-Time Postoperative Monitoring
Once the patient leaves the building, digital monitoring tools should take the wheel. These might include:
- Daily symptom check-ins (via app or text)
- Pain and medication tracking
- Smart alerts for signs of infection or poor mobility
- Video-based wound checks or telehealth follow-ups
With these tools, providers can step in before complications snowball.
4. Behaviorally-Informed Patient Engagement
Here’s where behavioural science shines. We know that recovery isn’t just physical—it’s emotional and psychological too. Good digital platforms use:
- Personalised nudges (e.g., “You’ve hit 80% of your recovery goals—great job!”)
- Gamified milestones (like earning badges for daily walks)
- Reminders tailored to the patient’s behaviour patterns
This isn’t just about fun—it’s about boosting compliance and reducing avoidable setbacks.
5. Analytics and Continuous Feedback
You can’t improve what you don’t measure. Digital recovery plans should track:
- Patient-reported outcomes (like pain or nausea)
- Adherence to the care plan
- Readmission rates and urgent care visits
- Patient satisfaction scores
With this data, ASCs can refine their workflows, train staff better, and demonstrate value to payers and accrediting bodies.
How Calcium Solves These Challenges
Let’s bring this all together. Calcium’s digital health platform is uniquely designed to help ASCs overcome these exact hurdles. Here’s how it stands out.
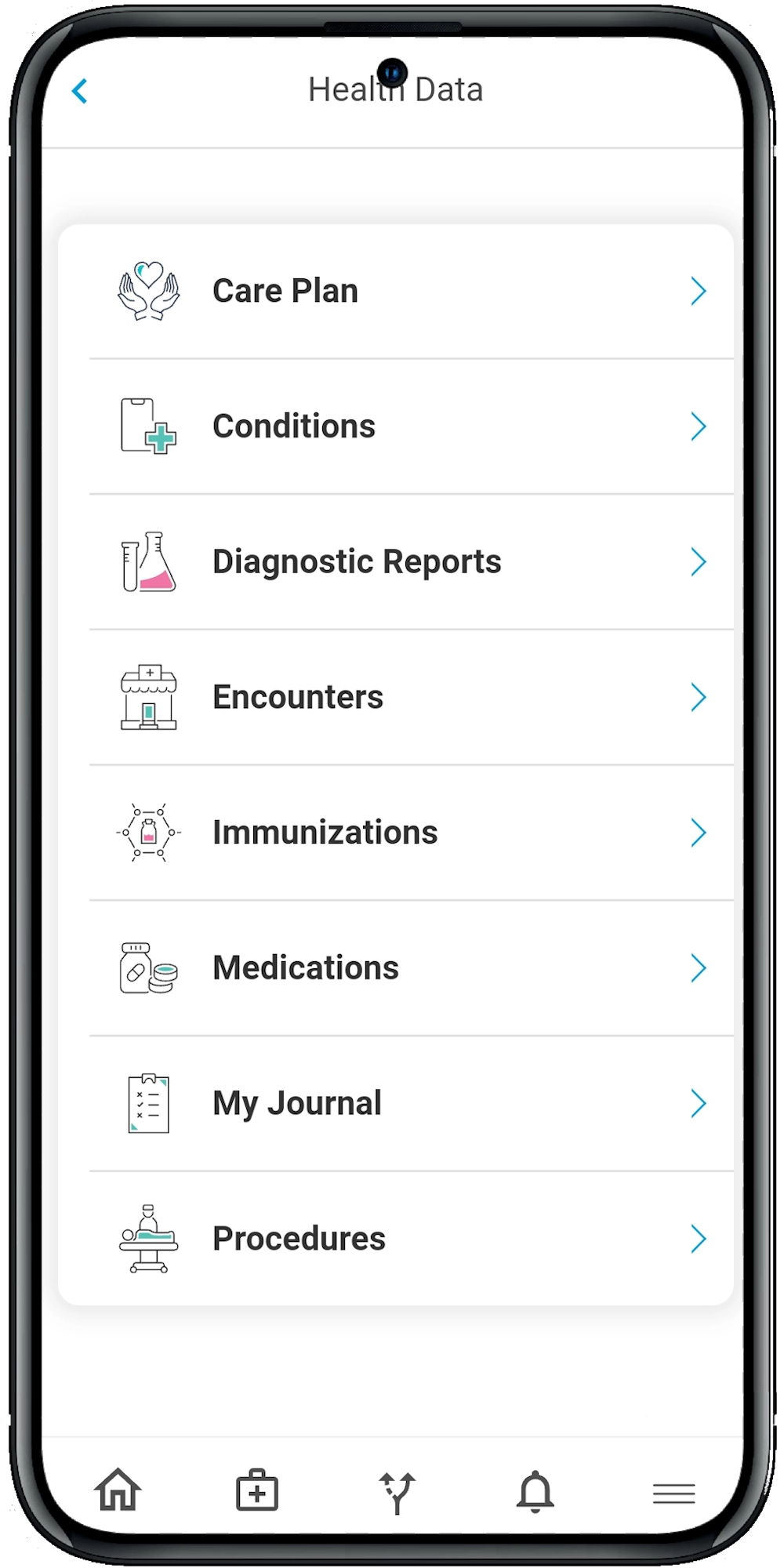
All-in-One Patient Recovery Hub
From pre-op prep to final follow-up, Calcium offers a single digital interface. Patients can view their care plan, check in with their provider, upload photos of incisions, or complete satisfaction surveys—all without bouncing between apps.
Real-Time Monitoring and Smart Alerts
Calcium pulls in real-time symptom data and flags problems before they escalate. For example, a patient reporting severe swelling or a pain score of 8+ triggers an alert to the surgical team—no guesswork involved.
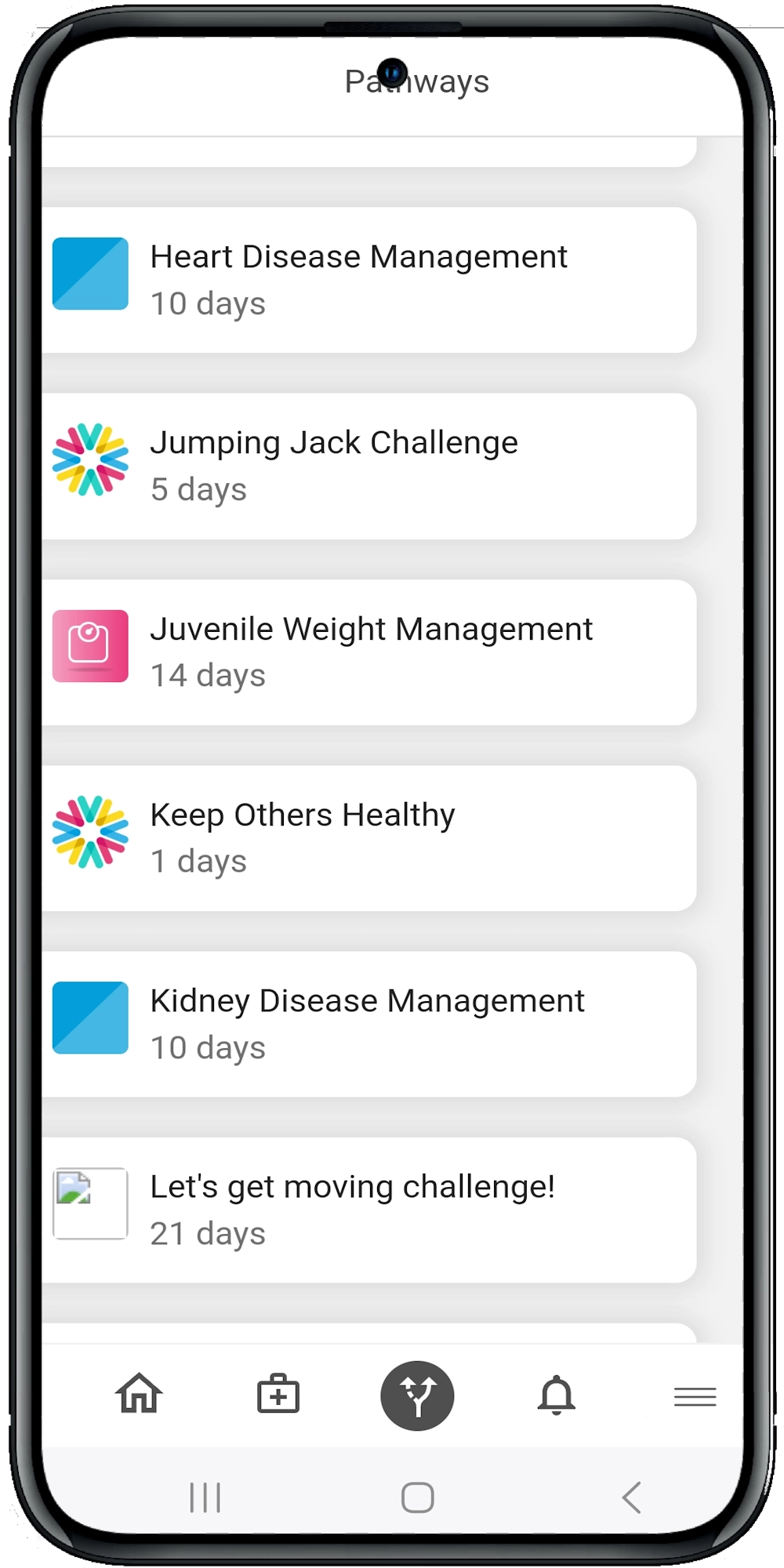
Behavior-Driven Engagement
Using behavioural health tools like journaling, motivational reminders, and mental health check-ins, Calcium helps patients stay on track emotionally as well as physically. This is especially valuable for recovery from surgeries that may impact body image, like mastectomies.
Data That Matters
The platform doesn’t just collect data—it makes it actionable. Dashboards show recovery trends, identify at-risk patients, and provide quality metrics that support value-based care contracts.
What’s Next?
Digital recovery plans aren’t a luxury anymore—they’re a necessity for ASCs that want to thrive under value-based care. And the good news? You don’t need to build it from scratch.
And recovery is no longer an afterthought—it’s a critical part of the patient journey that can make or break an ASC’s success. As value-based care reshapes the surgical landscape, digital recovery plans offer a clear path to better outcomes, higher patient satisfaction, and stronger financial performance.
But getting there takes more than good intentions—it takes the right tools. That’s where Calcium comes in. Our digital health platform is designed specifically for ASCs, helping you streamline recovery, monitor progress in real-time, and keep patients engaged every step of the way. Whether you’re looking to reduce readmissions, improve patient-reported outcomes, or simply modernise your care model, Calcium is here to help.
Reference
- Pai, S.-L., Ladlie, B., Locke, K., & Getting, R. G. (2024). Patient-Centered Care for Ambulatory Surgery. International Anesthesiology Clinics, 63(1), 14–22. https://doi.org/10.1097/aia.0000000000000461
- Allison, K. (2021). Assessing Transformation of Optimizing Ambulatory Surgery Center Services with Telehealth. MUSC Theses and Dissertations. https://medica-musc.researchcommons.org/theses/648/
- Afonso, A. M., McCormick, P. J., Assel, M. J., Rieth, E., Barnett, K., Tokita, H. K., Masson, G., Laudone, V., Simon, B. A., & Twersky, R. S. (2021). Enhanced Recovery Programs in an Ambulatory Surgical Oncology Center. Anesthesia & Analgesia, 133(6), 1391–1401. https://doi.org/10.1213/ANE.0000000000005356
- Afonso, A. M., Tokita, H. K., McCormick, P. J., & Twersky, R. S. (2019). Enhanced Recovery Programs in Outpatient Surgery. Anesthesiology Clinics, 37(2), 225–238. https://doi.org/10.1016/j.anclin.2019.01.007
- Wiggins, C., Peterson, T., & Moss, C. (2015). Ambulatory surgery centers׳ use of Health Information Technology. Health Policy and Technology, 4(2), 100–106. https://doi.org/10.1016/j.hlpt.2015.02.006